THE "SCHICK" INOCULATION FOR IMMUNISATION AGAINST
DIPTHERIA
An Exposure of its Dangers and Fallacies
M. BEDDOW BAYLY, M.R.C.S., L.R.C.P.
1939 2nd EDITION Issued by The National Anti-Vaccination League
(WHALE June 2002, Book supplied by John Wantling)
SECTION 1. THE GERM THEORY OF
DIPHTHERIA
SECTION 2. THE SERUM TREATMENT OF
DIPHTHERIA
EVIDENCE AGAINST THE USE OF SERUM
RECOGNITION OF THE FAILURE OF
SERUM WORLD-WIDE
CLAIMS VERSUS FACTS
SECTION 3. THE HARMFUL
EFFECTS OF SERUM TREATMENT
1.ANAPHYLACTIC SHOCK
2. SERUM DISEASE
3. REMOTE EFFECTS OF SERUM
ANTI-DIPHTHERITIC SERUM AS A
PROPHYLACTIC
SECTION 4. THE SCHICK TEST
1.THE
TEST IS OF NO VALUE IN CHILDREN UNDER FIVE (when it is most needed)
2.
THE TEST IS BEING ABANDONED IN NEW YORK AND OTHER PARTS OF AMERICA ON ACCOUNT OF ITS
UNRELIABILITY
2A.THE TEST HAS
ALSO BEEN DROPPED IN CERTAIN PARTS OF ENGLAND
3.
THE RESULTS OF THE TEST VARY ACCORDING TO THE FIRM SUPPLYING THE MATERIAL
4.
SCHICK-NEGATIVES MAY CONTRACT OR EVEN DIE FROM DIPHTHERIA
5. SCHICK-POSITIVE PEOPLE
DO NOT CONTRACT DIPHTHERIA
6.
RESULTS OF TEST IN LARGE NUMBERS OF SCHOOL CHILDREN IN CONFLICT WITH EXPERIENCE
7. SCHICK-NEGATIVE PERSONS MAY
BECOME POSITIVE
8. TEST OF NO VALUE BUT STILL
ADVOCATED
9. That the
Schick test alone may give rise to undesirable sequelae
ALLERGIC REACTIONS FOLLOWING THE
SCHICK TEST
SECTION 5. "SCHICK"
IMMUNISATION
THE FAILURE OF IMMUNISATION EVIDENCE FROM AMERICA FRANCE
GERMANY GREAT BRITAIN
IMMUNISED PERSONS CONTRACT DIPHTHERIA
EVIDENCE FROM AMERICA AMSTERDAM ENGLAND & WALES FRANCE IRELAND
ITALY SCOTLAND
IMMUNISATION HAS NO EFFECT ON
SEVERITY OF ATTACK
FALLACY UNDERLYING DESCRIPTION
"MILD."
FALLACY UNDERLYING FAVOURABLE REPORTS
GROWING
SUSPICION OF "SOMETHING WRONG" WITH THE METHODS
IMMUNISATION A PUBLIC DANGER
SPECIAL DANGER
TO INOCULATED CHILD WHO DOES NOT BECOME IMMUNE
COMPULSORY IMMUNISATION
SECTION 6. THE DANGERS
OF "SCHICK" IMMUNISATION
A SERIES OF DISASTERS 1919-1938
SECTION
7. THE INHERENT DANGERS OF "SCHICK" INOCULATION
TOXIN-ANTITOXIN TOXOID-ANTITOXIN (T.A.M.)
TOXOID-ANTITOXIN
FLOCCULES (T.A.F.)
TOXOID;
FORMOL-TOXOID (F.T.); RAMON’S TOXOID; ANATOXINE
ALUM TOXOID (A.T.) DIPHTHERIA TOXOID, ALUM-PRECIPITATED
(A.P.T.)
A TIMELY WARNING BY THE
"MEDICAL WORLD."
SECTION
8. DANGERS INHERENT IN ALL MIXTURES CONTAINING ANTITOXIN
DANGERS COMMON TO
BOTH TOXIN-ANTITOXIN AND TOXOID-ANTITOXIN
THE ARTHUS PHENOMENON
FREQUENCY OF REACTIONS
ACUTE
ANAPHYLACTIC SHOCK FOLLOWING INTRACUTANEOUS TEST FOR SENSITIVITY TO HORSE-SERUM
A MEDICAL OFFICER OF HEALTH’S
CHALLENGE
SECTION 9. STATISTICAL FALLACIES
1. ALTERATIONS IN DIAGNOSIS
A NEW NAME FOR DIPTHERIA IN THE
IMMUNISED
A COMPLETE VOLTE FACE
MILD CASES IN
"IMMUNISED" cannot BE DIPHTHERIA
TYPICAL
CLINICAL CASES NOT DIPHTHERIA IN "IMMUNISED" UNLESS KLEBS-LOEFFLER BACILLUS
PRESENT
2. ERRORS OF CLASSIFICATION
3. ERRORS DUE TO NATURAL
VARIATIONS IN INCIDENCE
4.
Some eminent bacteriologists do not accept the statistical method when dealing with
epidemics
SECTION 10. THE FALLACY
OF THE THEORY OF IMMUNITY
THE CAUSE OF DIPHTHERIA
THE PREVENTION OF DIPHTHERIA
HOW HEALTH DEPARTMENTS INSTIL
FEAR OF DISEASE.
SECTION
11. SUFFERING TO ANIMALS INVOLVED IN THE MANUFACTURE AND TESTING OF SERA
SECTION
12. WHAT EMINENT DOCTORS THINK ABOUT INOCULATION
ADVICE GIVEN BY THE MINISTRY OF
HEALTH
NOTE REGARDING THE USE OF THE TERM "SCHICK"
The qualifying adjective "Schick" is, strictly speaking, only applicable to the skin test which was devised by PROFESSOR BELA SCHICK, of Vienna, in 1913, and has consequently borne his name.
But the term has become, by popular usage, so closely associated with the complete process of testing and immunising that for the purposes of this pamphlet it seemed to be of advantage to use it throughout for the immunising inoculation as well for the preliminary test.
The reader will understand that wherever the term "Schick" occurs in inverted commas it is being used for convenience and not a strictly scientific sense.
NOTE TO SECOND AND REVISED EDITION.
In presenting this second and enlarged edition, the author wishes to make it quite clear that in no case does quotation from any authority imply that the writer is to be regarded as in any way opposed to orthodox principles of medical pathology and practice. Indeed, it is largely because the authorities quoted are of orthodox standing that the expressions of opinion extracted from their writings are the more noteworthy.
In regard to the criticism sometimes made that these quotations taken from their context create a false impression of the writer’s meaning, great care has been taken by the author to give sufficient context to render the quotations fair in this respect. Moreover, by giving the full page references the reader is encouraged, and is, indeed, urged, to study the original writings. For in most cases it has been impossible, for reasons of space, to do more than extract a more striking passage from among others of equal interest and importance.
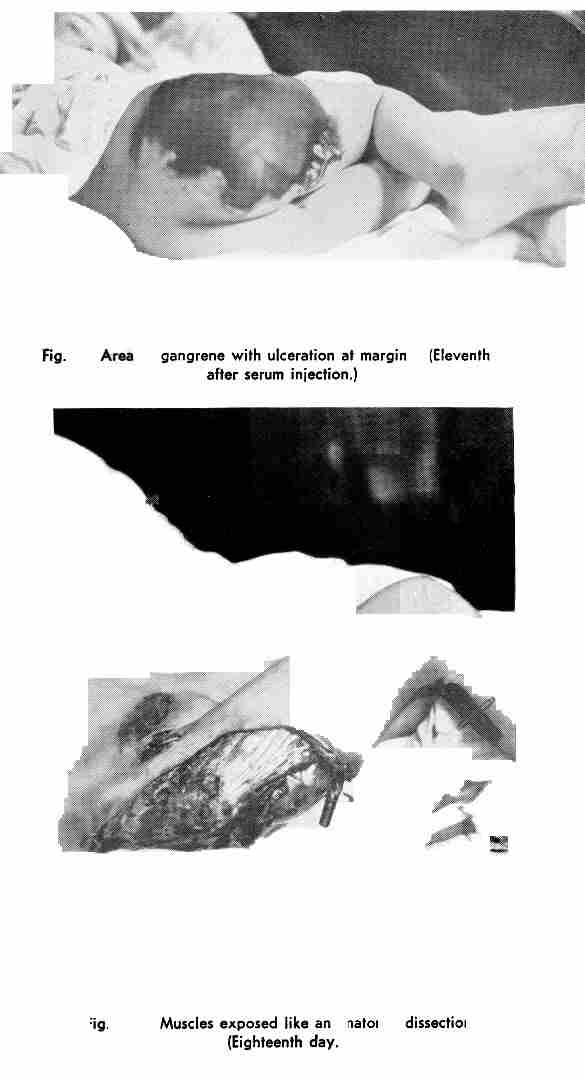
The author desires to express his indebtedness to DR. I. HARRISON TUMPEER and DR. H. E. IRISH, of CHICAGO, for the copies of their photographs from which the illustrations have been prepared, and for their kind permission to publish the same. Illustrations I, II and III appeared originally in the Journal of the American Medical Association, April 25th, 1931; illustrations IV, V and VI in the same Journal of February 18th, 1933.
SECTION 1
THE GERM THEORY OF DIPHTHERIA
The attempt in recent years to prevent diphtheria by the injection of toxin-antitoxin and similar products, as well as the routine treatment of diphtheria, when it occurs, by antitoxic serum, is based upon the primary fallacy that diphtheria is caused by a "germ"—the Klebs-Loeffler bacillus.
The following facts prove that this belief is a fallacy : —
1. The germ is absent in many cases of the disease it is alleged to cause:
In 14 per cent, of cases, according to the Lancet, Sept., 1898, (p. 779)
In 20 per cent. of cases, according to the Report of Royal Commission on Vivisection, 1912
(p. 38)
In 28-40 per cent, of cases, according to SIR WILLIAM OSLER (Principles and Practice of
Medicine, 8th Edition, 1912, pp. 58-60).
As the British Medical Journal, May 1st, 1926, quoting a Continental doctor, H. HECKSHER, stated: " Bacterial examination is not infrequently negative in just those cases of diphtheria which are most serious." (Epit. of curr. med. lit., p. 78.)
2. It is commonly present in many diseases it is not supposed to cause. A list of 17 of these, ranging from Eczema to Endocarditis and from Pleurisy to Puerperal fever, will be found in the Medical World (June 15th, 1928, p. 330).
SURGEON COMMANDER S. F. DUDLEY was reported in the Lancet, May 12th, 1928, as mentioning in the course of a lecture to the Society of Medical Officers of Health that " 15 per cent, of the swabs from over 1,000 non-membranous sore throats grew the Klebs-Loeffler organism." He went on to say that "the diphtheria throat swab had been in many ways a curse." For : —
"a positive report without a virulence or a Schick test must have forced a wrong diagnosis on many non-specific throats, thus falsifying the notification returns." (p. 965.)
3. It is frequently found in the throats of normal healthy people. According to the Ministry of Health Report (No. 10, p. 26), it has been demonstrated in 15 to 20 per cent. of school children.
The same Report (p. 14) states that in the Willard Parker Hospital in New York, of 1,200 patients, 20 per cent. had diphtheria bacilli in their throats and were in contact with diphtheria cases, and yet in no single instance developed diphtheria, although in many cases the bacilli were of a virulent type.
SURGEON COMMANDER S. F. DUDLEY found that "7 per cent. of some 4,000 healthy boys had been proved to be carriers at the (Greenwich) Royal Naval School." (Lancet, May 12th, 1928, p. 965.)
Even " persons giving a positive reaction (Schick)," and therefore supposedly susceptible to attack, " may occasionally harbour diphtheria bacilli in their throats without developing diphtheria." No explanation of this has been offered. (Report on Diphtheria, by the Ministry of Health, No. 10, p. 13.)
DR. MASSINGHAM, Resident Medical Officer at the London Fever Hospital, admitted in the Lancet, February 25th, 1928 :—
"A positive reaction with virulent diphtheria bacilli in the throat is compatible with perfect health." (p. 416.)
The Medical Echo, Vol. 14, No. 55, October, 1936, made an even more striking pronouncement in an article on "The Swab in Diphtheria," saying : —
"Persons may harbour virulent diphtheria organisms in their throat, and yield a Schick positive reaction and nevertheless show no signs of the disease clinically. Moreover, an investigation of their blood may show that there is no appreciable amount of antitoxin present." (p. 56.)
In fact, as DR. CLAUDE BUCHANAN KER, Medical Superintendent of the City Hospital, Edinburgh, wrote in his textbook, A Manual of Fevers (1912):—
"it is certain that a healthy mucous membrane is capable of resisting diphtheria and many persons in perfect health harbour the bacillus in the throat." (p. 224.)
4. The germs are innocuous when experimentally introduced into the healthy body.
(a) DR. RODERMUND "sprayed the poisons of diphtheria, smallpox, scarlet fever or consumption into the throat, nose [of his patients], or had them breathe into the lungs, repeating the experiments in most cases every one or two weeks for months with the result that no disease could be developed." (Medical Brief, St. Louis, U.S.A., 1906).
(b) DR. J. B. FRASER, of Toronto, and five volunteers swallowed millions of active Klebs-Loeffler bacilli in milk, bread, fish and alone, without any subsequent ill-effects (Canada Lancet, Vol. XLIX, No. 10, June, 1916, p. 447.)
(c) PROFESSOR UIRICH FRIEDEMANN, M.D., Berlin, has stated:—
"It is known that diphtheria bacilli do not live long in a healthy organism." (The Lancet, Aug. 4th, 1928, p. 214.)
5. It is clear that the claim of the Klebs-Loeffler bacillus to be considered the causal agent in the production of diphtheria is unsupported by scientific evidence. As PROFESSOR FRIEDEMANN affirmed when dealing with its almost ubiquitous nature:
"We came to the conclusion that in one year about one-third of the population is infected with diphtheria bacilli without contracting the disease." (Loc. cit.)
6. The part played by the bacillus in the transmission of the disease from one person to another is equally in doubt. For instance, the British Medical Journal, March 26th, 1927, reviewing an article on diphtheria which appeared in a Scandinavian medical journal, stated : —
"As in the observations of 1925-26 no case of clinical diphtheria developed in contact with any carrier, the author sees in this observation confirmation of the now general opinion that diphtheria carriers need not be isolated nor be the object of any special measures in the majority of cases." (Epit. of curs. med. lit., p. 57.)
PROFESSOR FRIEDEMANN reported that after investigation Doull and Lara:
"Came to the conclusion that the danger of infection by carriers is negligible compared with the danger of infection by patients." (The Lancet, Aug. 4th, 1928, p. 215.)
Furthermore, in regard to the latter he admitted that as the result of a League of Nations inquiry among seven different nations :
"We see that the number of case-to-case infections does not amount to more than 2.9 per cent, of the total diphtheria cases." (Loc. cit.)
The following annotation appears in the British Medical Journal, January 19th, 1935:—
T. Hünermann (Munch. med. Woch., October 20th, 1934, p. 1660) considers that the danger to the community of the diphtheria ‘carrier’ is apt to be grossly exaggerated. ….. He goes on to quote a statement made by Lenz that no case is known to public health authorities in which children, known to have been carriers for more than eight weeks, have infected a fellow pupil." (Epit. of curr. med. lit., p. 14.)
W. L. Scott, M.C., M.D., Second Medical Officer to the Post Office, reported in the Lancet, August 14th, 1937, the results of a careful investigation into the problem of "The Contact in Industry." With regard to diphtheria he found that, over a period of ten years, out of 7,697 contacts with the disease "only 1 contact in 274 (0.36 per cent.) subsequently developed the disease." (p. 398.)
7. No animal develops the signs and symptoms of diphtheria when experimentally injected with the germs. (Report of Royal Commission on Vivisection, 1912, p. 120.)
8. " Other microbes, such as the streptococcus, the tetragenus and the pneumococcus, take upon themselves occasionally to construct membranous formations on the tonsils . . . not to be differentiated clinically from diphtheria …. . they may be accompanied by glandular masses and suppuration." (The FrancoBritish Medical Review, Dec., 1924, Vol. I, No. 3, p. 47.)
The Kiebs-Loeffler bacillus, therefore, clearly fails to fulfil a single one of the conditions which would establish it as a causal agent in diphtheria, and were laid down as the essential requirements of the Germ Theory of disease by KOCH and PASTEUR, the originators of that theory.
In fact, the editorial of the Medical Officer, February 15th, 1936, contained the following remarkable statement : —
"The diagnosis of diphtheria rests with the physician, it cannot be made by the bacteriologist, who never professed that he could make it." (p. 61.)
This declaration is in striking contrast to that in OSLER’S textbook, The Principles and Practice of Medicine (8th Edition, 1912, p. 68), where it is stated:
"The diagnosis of the Klebs-Loeffler bacillus is regarded by bacteriologists as the sole criterion of true diphtheria, and as this organism is associated with all grades of throat affections, from a simple catarrh to a sloughing, gangrenous process, it is evident that in many instances, there will be a striking discrepancy between the clinical and bacteriological diagnosis."
SECTION 2
THE SERUM TREATMENT OF DIPHTHERIA
On this primary fallacy the whole case in favour of the treatment of diphtheria by antitoxic serum has been built up. SIR ALMROTH WRIGHT described such use of sera as resting, in his opinion, "on a foundation of sand." (Studies on Immunisation, 1909, p. 302.)
Anti-diphtheritic serum is manufactured by injecting a horse with increasing doses of toxin from the "germs," when, after several months’ interval, several litres of blood are drawn off from a vein in its neck.
The liquid portion, or serum, is separated off and is supposed to contain a substance, "antitoxin," which will neutralise the poison of diphtheria when injected into human beings.
Both the virulence of the toxin and the potency of the antitoxin are estimated and standardised by injecting them into guinea-pigs.
Since its introduction upon the market in 1894 this serum has been hailed as a triumph of the laboratory, which has "robbed diphtheria of its terrors." (see note) In reality it has proved a disastrous failure.
Note. In the Report of the Metropolitan Asylums Board for 1924-5 it is stated:— "There is a popular tendency to class diphtheria with scarlet fever, enteric fever, and certain other infectious diseases as one that modern medical science has definitely controlled and ROBBED OF MOST OF ITS TERRORS. That, however, is far from being the case." (p. 30.)
EVIDENCE AGAINST THE USE OF SERUM.
1. It is true that according to the Reports of the Metropolitan Asylums Board the death-rate per hundred cases declined from 30 in 1894 to 8.7 in 1922, but it had already fallen from 60 per cent. in 1888, seven years before serum was introduced. This prior fall in the death-rate remains unexplained.
Moreover, the fatality-rate in scarlet fever is shown by the same Reports to have declined far more over the entire period, and without the use of any serum.
Similar figures have been recorded in many parts of the world and the same arguments will be found to apply to them. Thus, DR. FRIEDBERGER maintained before the Berlin Medical Society, in 1931, that:—
"The remarkably favourable results that followed the introduction of antitoxin in the ‘nineties of last century were really due to a natural decline in the severity of the disease. As the result of a study of a large series of European and American statistics he had come to the conclusion that the diphtheria curve had been in no way affected by the introduction of antitoxin. . ." (The Lancet, March 14th. 1931, p. 598.)
2. The favourable statistics were brought about largely by the change of diagnosis from the clinical to the bacteriological.
"As a result of this change of view, cases of mild sore throat are now classed as diphtheria—cases which would, in any case recover, whatever the treatment; and the fatality of diphtheria will be reduced accordingly." (Editorial ill The Lancet, Nov. 4th, 1904, p. 1342.)
Recent confirmation of this is afforded by PROFESSOR W. W. C. TOPLEY, who, in his recent work, An Outline of Immunity (1933) refers to this change in the basis of diagnosis, and states:—
"For this reason, the total of recorded cases would tend to be increased by the inclusion of many mild infections, and the recorded case mortality would automatically fall. (p. 359.)
As a result, statistics of the case-fatality rates of diphtheria throughout the world have been invalidated. (See par. 2.)
3. On the other hand, the total deaths from diphtheria per million of the population increased after antitoxin was introduced: —
In the 30 years prior to 1894 (when serum was introduced) the deaths
from diphtheria in England and Wales were 4,676.
In the 30 years subsequent to 1894, the deaths were 5,197.
In the case of measles, whooping cough and scarlet fever the analogous
figures of mortality show, in comparison, a very large reduction; and this took place
without the use of any serum in these diseases.
4. The argument that the beneficial effect of serum is shown by the fact that the fatality-rate is least when the serum is given on the first day, and increases with delay, will be familiar to all.
No one, of course, would suggest that serum is deliberately withheld in order to prove this; the explanation is that cases in which there has been delay in giving the serum have not been diagnosed in the early stages or received appropriate nursing or other treatment, Obviously they would stand a worse chance of recovery.(Vide W, W, C, Topley: An Outline of Immunity (1933), p. 862.)
As the Medical Officer, March 9th, 1935, declared : —
"Even in diseases for which no specific treatment is available, early diagnosis may make enormous difference in fatality and complications, provided good nursing is available on diagnosis." (p. 92, col. i.)
Moreover, DR. GUNN, Medical Superintendent of Infectious Diseases Service, L.C.C., admitted in the Practitioner, October, 1934:—
"It is not rare to see a relatively early case—second or third day—in which membrane continues to spread In spite of huge doses of serum, even given intravenously." (p. 882.)
5. Finally, the claim that antitoxin has any beneficial effect at all on the fatality-rate is completely disproved by a comparison of the percentage of deaths among the inoculated with that of the uninoculated; the figures are given in the Retort of the Metropolitan Asylums Board for 1910, and show that during the previous ten years,
Among 50,405 cases treated with serum the deaths were 11.1 per cent.
whereas
Among 6,831 cases without antitoxin the deaths were 3.02 per cent.
The figures are all the more remarkable when it is realised that, according to this Report itself, cases too advanced to be given serum are included in the non-inoculated class.
It is also of interest to compare them with the case-fatality rates in other countries in recent years. The following figures were given in answer to a question in the House of Commons by the Minister of Health on July 31st, 1934:—
France (1931) 11.0 per cent.; Germany (1931) 7.1 per cent.; Poland (1933) 5.1 per cent.; Austria (1932) 4.6 per cent.; Belgium (1931) 22.6 per cent.; Denmark (1930) 2.7 per cent.; Spain (1933) 14.6 per cent.; Italy (1930) 11.6 per cent.; Norway (1931) 3.7 per cent.; Netherlands (1933) 4.5 per cent.; Sweden (1931) 3.6 per cent.; Switzerland (1932) 4.1 per cent.
In all these countries the routine treatment has included the administration of serum.
RECOGNITION OF THE FAILURE OF SERUM WORLD-WIDE.
So signal a failure has antitoxin proved to be in diphtheria that on all sides disappointment is being expressed by medical authorities. As DR. W. W. C. TOPLEY declared in his book, An Outline of Immunity. (1933): "Our confidence in the uniform efficacy of this form of treatment has been a little shaken by the happenings of recent years. In Germany and elsewhere there has been an increase in the frequency of severe and fatal cases that is not easy to explain." (p. 359.)
"There is a popular tendency to class diphtheria with .......other infectious diseases as one that medical science has definitely controlled and robbed of most of its terrors. That, however, is far from being the case, . . . the fact remains that for reasons not altogether clear, diphtheria appears to be strengthening its force and gathering power, unchecked by Science." (p.30)
2. DR. CAMERON KIDD, M.O.H. for Bromsgrove, declared himself "disillusioned" in the Brit. Med. Jour. of August 29th, 1925:—
"No one," he said, "will, I think, deny that the promise of twenty years ago, when antitoxin treatment was first adopted, that diphtheria mortality would be greatly diminished, has not been fulfilled." (p. 398.)
3. The Lancet, July 7th, 1928, in a leading article, referred to the early days of antitoxin when "there seemed no doubt that diphtheria was conquered," and confessed : —
"With the passing years these hopes have not been realised,….. . The incidence of diphtheria not only remains high, but in London, has for many years been steadily rising, whilst the case-mortality has shown an alarming increase in Germany and other countries where serum treatment has long been employed as a routine." (p. 21.)
4. The M.O.H. for West Lancashire Rural District reported in the Manchester Guardian of June 16th, 1930, that:
"never in the history of the Council’s Isolation Hospital had it been necessary to perform so many tracheotomies."
5. The Lancet of March 14th, 1931, reported " the extraordinarily severe epidemic of diphtheria which has recently occurred in Berlin and the high case-mortality in spite of the large doses of antitoxin given at an early stage of the disease." (p. 598.)
6. DR. FRIEDEMANN, of Berlin, was quoted in The Lancet of August 4th, 1928, as saying that the case-mortality of diphtheria used to be 4-7 per cent.; since 1926 it had risen to 25-35 per cent. "Even patients injected with large doses of serum on the first day," he declared, "have succumbed within 24 hours." (p. 212.)
7. The following Berlin letter, published in the Journal of the American Medical Association, May 9th, 1936, is so significant as to merit quotation in full : —
"Diphtheria, on account of the severe form in which it appears in Germany, is of particular concern to the pediatrician. Dr. Paschlau, staff member of a children’s hospital, addressed the Berlin Pediatric Society on diphtheria. The question as to the efficacy of serum has been brought to the fore. It is to be remembered that in 1913 Professor Bingel of Brunswick, with a vast amount of data at his disposal, was unable to distinguish appreciable difference between the effect of antidiphtheric serum and that of similarly injected plain horse serum (without antibodies). Since that time the sceptical have questioned the specific efficacy of antidiphtheric serum. After the war, diphtheria assumed a new character in many parts of Europe. Laryngeal diphtheria became less frequent, and since 1926 clinics in Berlin, Vienna, Düsseldorf and elsewhere have reported a great increase in cases of so-called toxic disorders of the naso-pharynx which, despite abundant dosage of serum, have shown a mortality of 40 per cent. or more. The amount of serum given has been increased; instead of from 200 to 500 antitoxic units per kilogram of body weight formerly employed, as much as 100,000 units came to be given and this dosage has been increased even to 800,000 units. Results from these massive doses are disappointing. Paschlau brought out that in these toxic states the antidiphtheric serum in large doses as well as in combination with antistreptococcus serum, blood transfusions, arsphenamine and in the form of symbiosis serum has been proved powerless. Paschlau next traced the decline in the value of serotherapy since the armistice, until now only on the first or second day of illness in toxic cases can even a modest degree of efficacy be anticipated. Few diphtheria patients, however, receive the serum at such an early stage." (p. 1674.)
8. The British Medical Journal, August 22nd, 1936 (Epit. of curr. med. lit., p. 29) gives a summary of an article by W. BEHR, which appeared in the Deutsche Medizinische Wochenschrift, May 8th, 1936 (p. 771); according to this writer the mortality among 253 toxic cases of diphtheria treated in the municipal hospital of Plauen was over 35 per cent., and the incidence of post-diphtherial paralysis 12 per cent.
9. The Medical World of April 29th, 1932, announced that diphtheria, save for the brilliant exception of America, is everywhere increasing in frequency and deadliness." (p. 159.)
10. The alleged brilliance of American success with serum is dimmed by the report in the New England Journal of Medicine, of February 1st, 1934 (p. 275). We are told in the editorial that:—
"There are, however, as the Bulletin of the Metropolitan Life Insurance Company points out, a number of States and large cities where the diphtheria death-rate is to-day not only disgracefully high, but actually increasing."
"The 1932 figure was actually 34 per cent, higher (in four States) than prevailed for the registration area of the United States for ten years previously."
11. DR. Louis COBBETT, in the Brit. Med. Jour. (July. 22nd, 1933) deplored the fact that antitoxin, so wonderfully effective in the laboratory, had had such a comparatively small effect in lowering the death-rate from diphtheria during the last 40 years. (p. 140,.)
12. At an inquest on a child of six who died from diphtheria at the isolation hospital at Thornton Heath, in spite of the early administration of serum, DR. F. TEMPLE GREY, pathologist, was reported in the Daily Telegraph, March 28th, 1934, as saying that:—
"Recently the mortality from diphtheria had been rising, despite the fact that antitoxin had been given. Recent work in England has confirmed the fact that a certain number of patients, even if antitoxin is given in time, die nevertheless."
13. There can be little doubt in anyone’s mind but that the reduction in case-mortality which occurred in the earlier years of this century can as reasonably be attributed to the increasing practice of sending cases into hospital, where they would receive adequate nursing, as to the routine use of serum. In his presidential address to the fever group of the Medical Officers of Health (Nov. 29th, 1935), DR. E. H. R. HARRIES was reported in the Lancet, December 7th, 1935, as stating that while he attached great value to the use of antitoxin he laid even more stress upon the importance of skilled nursing. The Lancet commented that" none will dispute that without skilled nursing, which ordinarily can only be obtained in hospital, antitoxin may be of little avail." (p. 1308.)
The foregoing authoritative evidence regarding the failure of antitoxin is a complete refutation of the claim made by SIR ARTHUR NEWSHOLME, K.C.B., M.D., F.R.C.P., in his book, The Story of Preventive Medicine. (1929.) He wrote : —
"The discovery of antitoxin for diphtheria was a triumph of laboratory research, the outcome of experimental work on immunity; the progress of this research can be seen from stage to stage, and it constitutes an epochal point in the history of medicine."
It will also be instructive to compare the statements in the preceding paragraphs 1 to 13 with that of WILLIAM J. MOORE, L.R.C.S., F.R.F.P.S., M.C.P.S., F.R.S.M., Examiner to the Scottish Nursing Council and late Surgeon to the Victoria Infirmary, Glasgow, namely, that : —
"As the result of Pasteur’s work, the mortality from ….diphtheria is today practically nil." (Medical World, May 8th, 1931.)
No more damning commentary on the fallacies and failures of such medical research (vivisection) and on the claims advanced by its votaries could be imagined than that afforded by the evidence contained in this pamphlet, which has been derived entirely from sources of unimpeachable authority.
SECTION 3.
THE HARMFUL EFFECTS OF SERUM TREATMENT
The following dangers are inherent in the practice of serum-therapy itself, and are not in any sense due to errors in manufacture, or storage, or of administration to the patient by the doctor.
They fall under three main headings: —
1. Immediate. This may take the form of sudden collapse and may sometimes be
followed rapidly by death.
2. Delayed. This may take the form of: (a) rashes, joint pains, etc., which may
occur after a few days; (b) a state of hypersensitiveness known as
"anaphylaxis," which may lead to severe illness, prostration and death.
3. Remote. This may take the form of numerous chronic and intractable types of
disease which, as often as not, are never traced to their true source.
Let us examine these in greater detail.
Many cases of sudden collapse and death in previously healthy individuals, following injection with serum as "contacts," have been recorded in the medical press ever since the classical instance of the death of DR. ROBERT LANGERHANS’ own son a few minutes after a prophylactic dose of anti-diphtheritic serum in 1896. (Serums, Vaccines and Toxins, W. CECIL BOSANQUET and J. W. H -EYRE, 1916, p. 126.)
In 1924 LAMSON collected data of forty-one similar deaths due to the administration of sera. (Journal of the American Medical Association, April 5th, 1924, p. 1091.)
In the Medical Press and Circular of January 19th, 1927, the statement is made that "It is almost always with anti-tetanic or anti-diphtheritic serum that fatal accidents or paralysis are observed." (p. 51.)
The Winnipeg Free Press, December, 1934, reported the death of a four-year-old child just 20 minutes after he had been given a prophylactic injection of anti-diphtheritic serum by DR. W. O. YORK, at the request of the parents.
The following two cases are recorded in order to show that not only anti-diphtheritic serum but scarlet fever antitoxin also may be responsible for sudden death when injected as a prophylactic.
There was recorded in the Lancet, October 20th, 1936, the case of a fourteen-year-old boy, an inmate of the Bramhope Branch of the National Children’s Home. It was reported at the inquest that he died within a few minutes of being given an injection of serum as a prophylactic against scarlet fever. (p. 897.)
Still more recently, the Northern Echo, November 22nd, 1937, reported an inquest at Newcastle-on-Tyne on a three-year-old boy who also died after an injection of scarlet fever antitoxin. The child had collapsed within a few minutes of the administration of the serum.
The foregoing are but a few isolated instances of "accidents" which have frequently been reported in the medical press. Warnings as to the dangers mentioned have from time to time been uttered by medical authorities. For instance, SIR WILLIAM WILLCOX, in an address to the Medical Society of London on October 12th, 1936, referred to the dangers of horse serum in the following words: —
"On giving serum for the first time it was necessary to inquire, if it was a foreign serum like horse serum, whether the person had had serum before and whether there was any evidence of allergy, such as urticaria. A very rare danger from serum was anaphylaxis, the patient dying within two or three minutes of the administration of the serum."
SIR WILLIAM WILLCOX went on to say that: —
"He had seen three deaths in exophthalnmic goitre after serum had been given for streptococcal throats. On the sixth day, when the serum fever occurred, these patients had a temperature, they had hyperthyroidism and the fever was followed by cardiac disturbance and death." (British Medical Journal, October 17th, 1936, p. 778.)
The risk of these serious effects of serum-therapy were again referred to in the Medical World. January 29th, 1937, in an article entitled "The Therapy of (Horse) Serum Reactions." The writer stated that " the person in whom allergic shock occurs almost always is one who is ‘naturally’ sensitive to horse serum. The person who is naturally sensitive to horse serum is one who is sensitive to horse dander." He warned his readers that: —
"Injection of horse serum into a person who is sensitive to horsedander and serum is an extremely serious undertaking. A reaction is practically certain to occur, even if the amount of serum administered is comparatively small. Large quantities of serum are likely to be extremely dangerous, and even one or two drops have been known to kill." (p. 769.)
(a) Serum Disease, which occurs in about 40 per cent. of the inoculated, has been investigated by many workers since it was first studied by VON PIRQUET and SCHICK in 1903-4. The widespread use of antitoxic serum in diphtheria has resulted in a large increase in the actual incidence of this condition according to DR. MITCHELL, who declared a few years ago that it was "evident that some factor is operating to cause an increase in the incidence of serum-disease, and that refinement of serum alone will not solve the problem " (my italics). (Journal of the Medical Society of New Jersey, January, 1930.)
In the Medical Press and Circular, January 19th, 1927 (p. 51), it is estimated that serum reactions occur in 12 to 15 per cent. of cases of children after the first injection, rising to 50 per cent, for subsequent ones, and in 75 per cent. of adults.
Even higher figures are mentioned in the Epitome of the British Medical Journal, December 31st, 1932 (p. 109). Statistics from a Chicago hospital, collected over a period of 19 years, show that reactions occur in 28.1 per cent, of cases with diphtheria antitoxin, 22.7 per cent, with scarlet fever antitoxin, and 81 per cent. with meningococcic serum.
The symptoms usually arise some three to fourteen days after the injection of the serum. They formed the subject of an interesting monograph in 1918 by DR. E. W. GOODALL, who collected and published observations on 3,500 cases of serum sickness following injections of diphtheria antitoxin. (The Lancet, March 2nd, 1918, p. 323.) [See also Article by PROF. BEZACON, Physician to the Hospital Saint Antoine, Paris in Franco-British Review, Sept., 1928, p. 263; also article on "The Nature and Clinical Significance of Anaphylaxis," by J. CHAMBSRLAIN, M.R.C,S., L.D.S., in The Medical World, January 2nd, 1~31 (p 469)]. They consist of rashes, generally urticarial in character, severe joint pains, glandular enlargement, abscesses at the site of the injection (even when strict asepsis has been observed), pyrexia, cardiac paralysis, vomiting and diarrhoea.
This same author, in A Textbook of Infectious Diseases (London, 1928), mentions 40.1 per cent, of rashes in a series of 8,726 cases examined; while DR. J. D. ROLLESTON, in Acute Infectious Diseases (London, 1929), refers to 66.4 per cent, of rashes among his 1,472 cases.
According to DR. J. H. WHITAKER, Medical Superintendent of the Grove Fever Hospital, London,
"The symptoms met with in serum sickness are now much more severe than in former times, especially in the case of adults. In addition to the usual well-recognised symptoms of serum sickness, it is now not at all uncommon to meet with vomiting and acute abdominal pain—two very unsatisfactory symptoms in diphtheria—and in a few cases I have lately met with haematuria, jaundice, extensive subcutaneous haemorrhages, and suppurative cervical adenitis. (Practitioner, Oct, 1926, p. 229.)
DR. L. J. WITTS, Assistant Physician at Guy’s Hospital, in the course of a clinical lecture delivered in January, 1931, on "Fallacies and Dangers in Treatment," referred to this danger in the strongest terms. Though an advocate of serum-therapy, he warned against the indiscriminate use of serum, for, he said : —
"You expose your patient to the risk of an immediate serum accident; you may inflict on him the painful disease of serum-sickness, in which the tortures of the cutaneous irritation, and the swollen joints may be almost unbearable, and finally you sensitise him to serum so that his life may be imperilled in the hour of need, when it may be essential to inject a potent serum," (Medical World, Jan. 23rd, 1931, p. 566.)
The last sentence of DR. WITTs’ warning brings us to the next danger.
(b) The first dose of serum, though causing no reactions of a severe nature itself, produces a condition in the patient of hypersensitiveness to any serum derived from the same animal; this condition is known as " anaphylaxis," and may result, when a second injection of serum takes place, in collapse or death of the patient, just as in the case of serum injected for the first time. (See under 1.)
Instead of collapse or immediate death, however, a condition may be locally set up at the site of the injection, which is known as the Arthus Phenomenon, and consists in mass gangrene of more or less extensive areas; this process will be found more fully described, with illustrations of actual cases which occurred as the result of the injection of TOXIN-ANTITOXIN, in the section which deals with the dangers of immunisation mixtures. (See p. 83 et seq.)
It is significant to find J. CHAMBERLAIN, M.R.C.S., L.D.S., declaring before Guy’s Hospital Physical Society in 1931, that:
"The increasing frequency with which human interference permits injections of antigenic substances into the circulating blood, betokens an increasing number of fatal anaphylactic reactions and other less significant forms of sensitisation." (Medical World, Jan. 2nd, 1931, p. 476.)
There can be no reasonable doubt but that the increasing practice of immunisation against diphtheria has increased the incidence of serum reactions. H. A. RAEBURN, M.D., M.R.C.P., D.P.H., writing on diphtheria immunisation in the Lancet, September 11th, 1937, recalled that GORDON and CRESSWELL recorded, in 1929, serum reactions in 74.1 per cent. of scarlet fever cases who had previously been immunised against diphtheria, when treated with serum, and only 18 per cent. in nonimmunised individuals. (p. 623.)
In the British Medical Journal, June 8th, 1935 (Epit. of curr. med. lit., p. 92), reference is made to an article by J. G. J. BATAILLE (These de Paris, 1985, No. 3), in which are recorded 15 cases of paralysis following and due to the use of diphtheria antitoxin. The onset is characterised by violent pain during the course of typical serum sickness 8 to 10 days after inoculation. Complete recovery is the rule, but takes place very slowly."
Recently, HILDA M. DAVIS, M.D., D.P.H., undertook the analysis of 4,835 consecutive cases of serum inoculation for diphtheria, during the period 1929-33, at the North-Western (L.C.C.) Hospital, London (The Lancet, Jan 22, 1938, p193).
She found that 21.9 per cent. gave reactions, of which 2.9 per cent, were local and 17.5 per cent, general, the remaining 1.5 per cent. having albuminuria only. Albuminuria was present in 2.8 per cent. of all cases treated with serum and was present in 13 per cent, of all cases of reaction. Children under five years of age showed the most frequent reactions. On the whole, these results were similar to those found by L. W. HUNT in his cases at the Durand Hospital, Chicago, in 1932. He reported in the Journal of the American Association, 99, 909, that 28.1 per cent. of the 2,859 cases developed rashes.
DR. H. M. DAVIS’s investigations showed there was evidence that different batches of serum varied in their power to provoke reactions, a phenomenon which caused DR. H. STANLEY BANKS, at a meeting of the Fever Group of the Society of Medical Officers of Health on November 80th, 1934, to declare : —
"The suggestion that certain horses appeared to give a toxic serum was one that called urgently for investigation."
The more remote effects of serum inoculation have been emphasised by J. E. R. MCDONAGH in his most recent writings. His unique work on the chemico-physical properties of the blood, especially in regard to the colloidal protein particles, is worthy of the closest study. One of his particularly pertinent statements is as follows:—
"Serums are very liable to give rise to shock, and to the more obvious manifestations produced the term ‘anaphylaxis’ is usually applied. Owing to the peculiar constitution of the protein the appearance of the signs and symptoms of shock may be delayed months and even years, and the longer the delay the more difficult grows the problem of combating them. The long delay frequently results in the manifestations of chronic disease, which, as often as not, remain for ever unconnected with the cause. When death occurs, it does so slowly, and after a long period of time (My italics.) (Nature of Disease Journal, Vol. 2, 1933, p. 126.)
Arising out of the condition of sensitisation, or anaphylaxis, which, it is admitted, is induced in greater or less degree in all who are injected with animal serum, there comes about an even more serious, because more subtle, danger. For, even if no further injections of serum are administered for other diseases, or prophylactically after accidents (for tetanus), this "allergic " state of the body may be one of the most important factors in predisposing the person concerned to the development of malignant disease.
This is not the place to discuss the investigations of WM. FREDERICK KOCH, M.D., D.Ph., of Detroit, in connection with the basic principles underlying all types of allergy, among which he classes not only over-secretion as in hay-fever, and over-contraction of muscle, as in asthma, but over-function of the process of cell-division and growth which is characteristic of cancer.
Suffice it to say that any substance which, when introduced into the body, can produce allergic sensitivity, does so by virtue of its power to inhibit normal oxidation-processes and thus render cell-function "irrifable" and liable to over-stimulation. The extra stimulus needed is provided by the power these substances possess of conveying energy, in the form of radiation, to the cells, and thus stimulating the particular vital function of the cells with which the transferred radiation is in "resonance." Thus it may be secretion, spasm, tumour, or finally ulceration which is the morbid manifestation of the underlying sensitisation. Those desiring more details of DR. KOCH’S illuminating work should consult his writings [See The Medical World, March 10th, 17th and 24th, 1989: "Pathogenesis and Immunity," by Wm. F. Koch, M.D., Ph.D.]
The important point to bear in mind is that among the many forms of chronic disease which, as J. E. R. MCDONAGH points out, remain for ever unconnected with the cause," namely, animal sera, we must include the greatest scourge of all, cancer, and other types of malignancy. [The length of time that may elapse before malignancy asserts itself presents no scientific obstacle to its credibility. It has been found that a radio-active substance, thorium dioxide, definitely causes bone-tumours in workers who have handled the substance for many years. Writing of the possible danger of a similar substance, thorotrast, giving rise to malignant tumours in man when injected for the purpose of taking X-ray photographs, W. E. Gye, M.D., F.R.S., states that "a period of ten or fifteen years might be expected to elapse before thorotrast produced a tumour in man." (86th Annual Report of the Imperial Cancer Research Fund, 1987-38, p. 7.)]
ANTI-DIPHTHERITIC SERUM AS A PROPHYLACTIC.
Many years ago, before the introduction of modern " immunising" preparations, the injection of antitoxic serum itself was practised as a preventive of infection in " contacts." The chief objection to its use was that the passive immunity alleged to be conferred by the serum was admittedly of very short duration— not more than about three weeks [In the British Medical Journal, November 25th, 1933, E. G. Munro Jones, M.R.C.S., L.R.C.P., and John D. KERSHAW, M.B., B.S., D.P.H., write: —"The incidence of diphtheritic infection in passively immunised patients . . . would suggest that it is unwise to regard this form of immunity as lasting more than three weeks." (p. 970.)] Four cases of diphtheria within 15 days of inoculation are recorded.
(1) DR. MENTON, in an article in the British Medical Journal, August 10th, 1935, entitled "Some Immunological Aspects of the Cure and Prevention of Diphtheria," draws attention to some other drawbacks. He says: —
"Its use for this purpose merely gives a false sense of security; sensitises the patient and increases the risk of unpleasant reactions if he should afterwards need serum treatment; may lead to a higher carrier rate; and may delay the development of natural active immunity." "(p. 246.)
Altogether, a catalogue of disadvantages which one would think would have completely discounted any usefulness its most enthusiastic supporters could ascribe to it.
(2) In an article entitled "Active Immunisation against Tetanus," published in the British Medical Journal, March 6th, 1937, HERBERT H. BROWN, O.B.E., M.D., F.R.C.S., points out the "serious disadvantages" of passive immunisation with antitoxin. He says: —
"Another serious drawback is the sensitization to horse serum, which to a greater or less degree follows immunization with antitoxin derived from immunized horses, a sensitization continuing for many years. Troublesome serum reactions, and even severe and in some cases fatal anaphylactic shock, may accompany or follow the subsequent injection of a therapeutic serum which may be urgently needed in the treatment of an infection such as diphtheria." (p. 494.)
If the reader will turn to the chapter which deals with present-day immunising mixtures, he will find that what DR. J. MENTON alleges in regard to the now discarded prophylactic serum is also true, in the opinion of the authorities quoted, of the succession of modern injections which have within recent years emerged from the laboratories of the manufacturing chemists. DR. HERBERT H. BROWN’s description of the serious drawbacks involved in sensitisation by serum is equally applicable to those modern preparations which contain antitoxin as an ingredient; instances of the unfortunate results which have followed their use will be found in section VIII.
SECTION 4
THE SCHICK TEST
The Schick test consists in injecting a small quantity of the toxin of the Klebs-Loeffler bacillus into the skin, and is therefore based on the fallacy that the germ is the cause of the disease.
According to a Memorandum drawn up by DR. KER, Medical Superintendent of the Edinburgh City Fever Hospital,
"By the use of a simple test, it is possible to find out those children who are liable to take the disease and those who are not." (The Lancet, Nov. 8th, 1924, p. 950.)
A positive reaction, it is claimed, indicates susceptibility; a negative reaction, immunity from diphtheria.
It should be particularly noted, however, that DR. R. C. O’BRIEN, at the summer meeting of the Association,of Clinical Pathologists in Eastbourne on July 20th, 1935, stated that: "There was no absolute line of demarcation between Schick-positive and Schick-negative individuals."
1. THE TEST IS OF NO VALUE IN CHILDREN UNDER FIVE (when it is most needed).
DR. J. A. NIXON, Physician to the Bristol Infirmary, stated that:
"The (Schick) test was of no value in children under five years of age . . . and it gave no evidence as to the virulence or avirulence of any infection." (Brit. Med. Jour., July 7th, 1923, p. 20.)
We find DR. LOUIS VAN BOECKEL reporting to the League of Nations Health Organisation in 1924 that:
"The tendency at present (in America) is to omit the preliminary Schick test."
The following year, 1925, the Annual Report of New York City declared that the test had been abandoned (p. 114).
In an article entitled "Should the Schick Test be Abandoned? " in the American Journal of Public Health, October, 1925, WILFRED H. KELLOGG, M.D., Director of the Bureau of Communicable Diseases, California State Board of Health, pointed out that "The percentage of error in reading reactions in those who are protein sensitive is, in the hands of even the most experienced, frequently as high as 50 per cent."
In the (American) Medical Journal and Record, March 3rd, 1926, it is stated : —
"There is a growing feeling among Public Health workers that the Schick test should be abandoned in the immunization of large groups of children. In fact, there are those who believe it is a useless procedure both in private and public health practice." (p. 332.)
2A. THE TEST HAS ALSO BEEN DROPPED IN CERTAIN PARTS OF ENGLAND.
In Birmingham, according to a report in the Lancet, November 24th, 1934, the Schick test was abandoned in 1931 owing to the doctors feeling that they "could not take the responsibility of assuring persons that a Schick-negative reaction indicated a complete and permanent immunity to diphtheria." This decision was evidently prompted by the occurrence of two fatal cases of diphtheria in Schick-negative children in 1930-31.. (p. 1182.)
In 1934 it was proposed to dispense with the routine preliminary Schick test in Kensington on the ground that the reaction is positive in practically every child under five, and that the majority of children under twelve are susceptible.
In Lincolnshire the Council decided to dispense with the Schick test entirely, and only undertake sample testing in the I to 1 1/2 year group.
In an article on "The Present Position of Diphtheria Immunisation" in the Medical World, March 1st, 1935, Dr. Elwin Nash, Medical Officer of Health for Heston and Isleworth, stated his opposition to " the advice of the League of Nations and the Army Authorities that the preliminary testing is unnecessary," and to their " not insisting on the posterior Schick." (pp. 11, 12.)
3. THE RESULTS OF THE TEST VARY ACCORDING TO THE FIRM SUPPLYING THE MATERIAL.
DR. PETERS, of Bristol University, found that test material from two different firms, when tried on the arms of 11 individuals, gave in one case 8 positive reactions and 3 negatives; in the other, 5 positives and 6 negatives. An alarming disparity," he remarked. (The Lancet, October, 6th, 1923, p. 784.)
4. SCHICK-NEGATIVES MAY CONTRACT OR EVEN DIE FROM DIPHTHERIA.
J. WUSTENBERG writes from the Robert Koch Institute in Berlin:
"Schick himself was of the opinion in 1922 that a negative Schick test put diphtheria out of court; but several writers have reported cases of diphtheria in which the Schick test was negative." (British Medical Journal, Oct. 31st, 1936; Epit. of curr. med. lit., p. 69.)
DR. FORBES, in his book, Diphtheria, Its Distribution and Prevention (1932), admits that : —
"The immutability of the negative reaction is not always to be ‘depended on as a constant index of immunity." (p. 809.)
He goes on to say that:
"Results, which have been accumulating during recent years, have shown, notably in the case of Schick-testing of members of Hospital nursing staffs, that occasionally primary Schick-negatives, and those who have been immunised and have subsequently yielded a negative reaction, may contract diphtheria." (pp. 809-10.)
In DR. FORBES’S records there are 115 cases of diphtheria in primarily Schick-negative persons, and 31 cases in persons found to be Schick-negative after a course of three or more injections.
DR. WILLIAM ROBERTSON, in his Annual Report for Edinburgh (1927), reported 58 cases of diphtheria among Schick-negative children.
The British Medical Journal, July 17th, 1926 (Epit. of curr. med. litt., p. 9), quotes from a Munich medical journal a doctor who "has recently observed 12 cases of diphtheria in children with a negative Schick reaction."
DR. MASSINGHAM, R.M.O. of the London Fever Hospital, reporting on four nurses who, although tested and found Schick-negative (two immunised), developed diphtheria, concludes that: —
"There are people who, although susceptible to diphtheria, may yet give a negative Schick reaction." (The Lancet, Feb. 25th, 1928, p. 416.)
According to an article by H. J. PARISH, M.D., M.R.C.P., D.P.H., and JOYCE WRIGHT, B.M.Oxon., in the British Medical Journal, March 16th, 1935:—
"Dudley, May and O’Flynn (1934) described an epidemic of 23 cases of mild diphtheria . . . at Greenwich Hospital School; 19 of the 23 patients had been Schick-negative either at the onset of the attack or in the previous two years."
"Robinson and Marshall (1934), working in Manchester, found 12 diphtheria patients who had negative Schick reactions immediately prior to the onset of the disease; one case was recorded as ‘ severe,’ 3 as ‘ moderately severe,’ and 8 as ‘ mild
Recording their experience at a residential school near London which between 1931 and 1934 had been thoroughly immunised, they stated : —
"The epidemic started in July, 1934, in newcomers who had already been attacked by measles and other infectious diseases, and spread to the rest of the school. Altogether there were 4 cases in unimmunised subjects, and 8 in children Schick-negative, either naturally or after a course of immunisation." (p. 601.)
They concluded that : —
"There is no doubt that, coincident with the increased prevalence and severity of diphtheria in many areas in England, the number of cases reported in Schick-negative reactors has also tended to increase." (Loc. cit.)
In the Lancet, August 24th, 1935, D. T. ROBINSON, M.Sc., M.R.C.S., and F. N. MARSHALL, M.D., D.P.H., writing of the incidence of diphtheria in Manchester, stated : —
"In the present series of cases we have encountered a further 13 instances of clinical diphtheria in persons in whom the Schick reaction was negative at the onset of the illness. Twelve of these were natural Schick-negatives, and one, a nurse, had been immunised with three 1 c.cm. injections of toxoid-antitoxin floccules (T.A.F.) three years previously and had been Schick-negative when tested six months later. She was still Schick-negative when tested on the day the illness began.
"While these cases were for the most part mild or moderately severe, it will be noticed that 3 are described as severe and 2 of these patients died from toxiemia." (p. 443.)
In order to escape from this difficulty and suppress evidence unfavourable to immunisation, authorities have even gone so far as to invent a new name for diphtheria when it occurs in persons "who had at one time or another been Schick-negative." According to H. J. PARISH, M.D., M.R.C.P., D.P.H., of the Wellcome Research Laboratories, the disease is to be called "TONSILLITIS IN SCHICK-NEGATIVE CARRIERS." (Lancet, March 16th, 1935, p. 600.) [See under Statistical Fallacies, Section IX, p. 95.]
5. SCHICK-POSITIVE PEOPLE DO NOT CONTRACT DIPHTHERIA.
(a) According to the Ministry of Health Report on Diphtheria, No. 10:—
……persons giving a positive reaction may occasionally harbour diphtheria bacilli in their throats without developing clinical diphtheria." (p. 13.)
No explanation of this anomaly has been offered.
(b) DR. MASSINGHAM, Resident Medical Officer of the London Fever Hospital, writing in the Lancet, February 25th, 1928, admitted that
"All Schick-positive people, although constantly exposed to massive doses of infection, do not contract diphtheria: and that a positive reaction with virulent diphtheria bacilli in the throat is compatible with perfect health." (p. 416.)
(c) Writing in the Medical Officer, October 12th, 1935, DR. PHILIPS COLE, M.O.H. for Beckenham, drew attention to the fact that:—
"The schools with the lowest degree of natural immunity [as shown by a Schick-positive reaction] consistently suffer far and away the least from diphtheria in times of increased prevalence." (p. 160.)
(d) The Medical Officer, December 14th, 1935, declared in a leading article on" Diphtheria Immunisation in Rural Districts":
"We know that Schick positives do not necessarily develop diphtheria, in fact only about 25 per cent. of them do so." (p. 241.)
(e) The Medical Echo, Vol. 14, No. 55, October, 1936, contains an article on "The Swab in Diphtheria," which concludes with the statement:
"Persons may harbour virulent diphtheria organisms in their throat, and yield a Schick positive reaction and nevertheless show no signs of the disease clinically. Moreover, an investigation of their blood may show that there is no appreciable amount of antitoxin therein. It is therefore obvious that there must be some other factor in immunity against diphtheria, besides the circulating antitoxin. (Proceedings of the Royal Society of Medicine, March, 1936)." (p. 56.)
6. RESULTS OF TEST IN LARGE NUMBERS OF SCHOOL CHILDREN IN CONFLICT WITH EXPERIENCE.
It is claimed that as a result of tests in this country and America, the children of better-class households are more susceptible to infection than those of the poorer classes, since the latter gradually become immunised through constant contact with infection.
Tests carried out on large numbers of school children in 16 different types of school by W. T. BENSON, M.D., D.P.H., Assist. M.O.H. for Edinburgh, and reported in the Lancet, November 8th, 1924 (p. 952), showed that children attending the schools serving the better-class neighbourhood were over two and a half times as susceptible to diphtheria as those coming from a slum area.
The logical conclusion to be drawn from this would be to encourage the slums and pull down the better-class houses, in order to increase resistance to infectious disease. The manifest absurdity of this whole theory is borne out by vital statistics, e.g. : —
(a) G. CHESNEY, M.B., B.Ch., D.P.H., gives the following result of Schick tests (Medical World, May 13th, 1932, p. 206):—
Poole elementary school children: 18.7 per cent, negative (insusceptible).
London elementary school children: 54.27 per cent. negative.
Yet we find the less susceptible schools have higher attack-rates : —
Diphtheria attack-rate (average) per 1,000 in Poole:
in 1911-20 1.48
in 1921-28 0.57
Diphtheria attack-rate (average) per 1,000 in London:
in 1911-20 3.05
in 1921-28 2.86
(b) The Registrar-General in his Statistical Survey for 1930 gives the following comparative figures for incidence of diphtheria:
Cases under 15 per 10,000 population in London...... 132
in county boroughs . .. 83
in other urban districts... 70
in rural districts....... 50
He comments : —
"It will be seen that the excess of prevalence in London falls into line with large excess for great towns over small, and for small towns over rural areas, in all parts of England." (p. 42.)
This disproves the theory that crowded conditions provide a natural immunity through "contacts."
(c) AUSTIN PRIESTMAN, M.B., D.P.H., M.O.H. for Folkestone, writing in the Medical World, February 6th, 1931, on the incidence of diphtheria in schools, states that it was observed to be highest "in those schools where sanitation is most deficient and ventilation and lighting the least satisfactory. The brightest and airiest school showed the least incidence, and the incidence throughout all the schools placed them in exact order of sanitary virtue. Moreover, the incidence indicated the schools where malnutrition in the children is most conspicuous." (p. 627.)
7. SCHICK-NEGATIVE PERSONS MAY BECOME POSITIVE.
(a) AUSTIN PRIESTMAN, M.B.~ D.P.H. (in the Medical World, February 6th, 1931), writes:—
"This would seem to point to the conclusion that a Schick-negative can become Schick-positive, and is now doing so with greater frequency than we have hitherto imagined possible." (p. 627.)
(b) DRS. YOUNG and CUMMINGS, in the Journal of the American Medical Association (February 18th, 1933, p. 530), maintain that
"Both artificially produced negatives and natural negatives tend to become positive over a given period of time."
(c) DR. MATTHEW BURN, Chief Assistant Medical Officer of Health for Birmingham, and DR. VERA FELLOWES, Assistant Medical Officer for Immunisation and Maternity and Child Welfare, described in the Medical Officer, July 11th, 1931, their experiences in the re-testing of Schick-negative children in schools. They wrote:—
"Do we not see that some 50 per cent. of children who on a given date are primary negative reactors, and therefore, hitherto considered immune, may when tested at a later date, show positive reactions? Can any great reliance be placed, therefore, on the interpretation of the reading of the test, as indicating permanent immunity……?" (pp.15-1G.)
(d) In the Editorial of the British Medical Journal, June 16th, 1934 (p. 1082), we may read :—.
"Ten per cent, of boys artificially made Schick-negative may become Schick-positive in from six months to four years . …"
(e) DRS. H. J. PARISH and J. WRIGHT refer in the Lancet, March 16th, 1935, to the fact that Parish and Okell (1928) found that 5 per cent. of children Schick-negative after immunisation had reverted to Schick-positive one to seven years later. (p. 603.)
(f) In an article on "Public Health in the U.S.A.", in the British Medical Journal, October 3rd, 1936, RALPH M. F. PICKEN, M.B., Ch.B., B.Sc., D.P.H., Mansel Talbot Professor of Preventive Medicine, the Welsh National School of Medicine, confessed: —
"In some areas, however—for instance, Chicago—a rather disappointing percentage of immunised children have been found to have relapsed to Schick-positive some years after immunisation." (p. 679.)
8. TEST OF NO VALUE BUT STILL ADVOCATED.
J. E. R. MCDONAGH, F.R.C.S., in the Nature of Disease Journal (Vol. I, 1932, p. 148), declares:—
"The most commonly performed immunity reaction is the skin test, which depends upon the production of a wheal . . . the test is of no value."
In spite of all this, Messrs. Burroughs, Wellcome and Co., in their recently-issued directions (6689H/J.786) for using their diphtheria prophylactic, make the statement that : —
"It is never safe to assume immunity after immunisation unless proved by a subsequent Schick Test."
Recently, too, DR. W. A. MURPHY, M.O.H., writing in the Medical Officer, July 21st, 1934, stated:—
"Diphtheria immunisation without re-testing is not a scientific procedure and should not be practised." (p. 29.)
More recently still, DR. Guy BOUSFIELD, in a letter to the Vaccination Inquirer, January 1st, 1936, said : —
"My criterion of immunity is a negative Schick test."
On the other hand, medical officers and bacteriologists of equal experience have come to diametrically opposite conclusions. For instance, PROFESSOR W. W. C. TOPLEY, in his book, An Outline of Immunity (1933), states: —
"We should never accept the proof that active immunisation will convert a Schick-positive to a Schick-negative reactor as final evidence that this procedure will protect against natural infection." (p. 329.) [See page 29, par. 2a, ante]
DR. J. C. SAUNDERS, M.O.H. for Cork, writing in the Medical Officer, December 28th, 1935, says that he agrees with the editor of the Medical Officer that: —
"the conversion of a positive to a negative reaction should not be the criterion and that the real test is protection from diphtheria." (p. 269.)
In an article on " Diphtheria—A Preventable Disease," by J. G. FITZGERALD, M.D., D. T. FRASER, M.D., N. E. MCKINNON, M.D., and MARY A. Ross, from the School of Hygiene and Connaught Laboratories, University of Toronto, the conclusion is reached that:—
"Requirements for the Schick test are in need of revision and standardisation. It is not infallible and its limitations should be recognised." (The Lancet, February 12th, 1938, p. 396.)
9. That the Schick test alone may give rise to undesirable sequelae if the body has already been sensitised by some previous inoculation does not appear generally to be realised, but evidence of this fact is accumulating.
As DR. H. J. PARISH stated in the Lancet, August 8th, 1936:—
"It is not generally. recognised that so trifling a procedure as a Schick test may be followed by some degree of allergic manifestations." (p. 310.)
ALLERGIC REACTIONS FOLLOWING THE SCHICK TEST.
(a) It will be remembered that in this country, according to the Report on Diphtheria (No. 10, 1921), issued by the Ministry of Health, the original strength of toxin advocated by Schick is not used. Instead, a solution of half this strength was adopted, the reason " being found in the fact that reactions obtained in susceptible individuals with this dilution of toxin tend to be less severe and persistent than when the more concentrated dilution as originally employed by Schick, is employed." (p. 15.)
(b) DR. C. C. OKELL referred in the Bulletin of Hygiene, July, 1934, to a Paper by J. D. MONROE and V. K. V0LK, in collaboration with W. H. PARK, in which are recorded reactions from Schick tests in two children who had previously been immunised with toxoid. In one case, a boy of ten, within half an hour the lips and eyelids became swollen and the child became cyanotic and short of breath. Urticaria appeared over the entire body. The other case was similar; in a child of three, within ten minutes of the Schick-test injection there developed urticaria over the whole body, extreme restlessness, shortness of breath, cyanosis, coughing, vomiting, swelling of the eyelids and lips.
(c) H. J. FREEDMAN reported in the Journal of Pediatrics, May, 1935 (p. 695), two cases in female infants, aged 11 and 12 months respectively, who, having previously been immunised with toxoid, developed generalised utticaria immediately following an injection of Schick toxin. In one case there was laryngeal stridor and cyanosis.
(d) DR. JOYCE WRIGHT reported in the British Medical Journal, May 4th, 1935 (p. 949), an instance of loss of sensation in the arm, which developed about five weeks after a Schick test injection, Eventually the area of loss of sensibility to heat, cold, etc., extended down to the wrist and remained for several weeks.
A similar case was reported in the British Medical Journal, February 16th, 1935 (p. 331), by DR. R. MILES ORPWOOD; further reactions were reported in the British Medical Journal on May 18th (p. 105), by DR. R. J. TOLEMAN, of Oxford, and on May 25th, 1935 (p. 1100), by DR. LYDIA M. HAUGHTON.
(e) In the Lancet, August 8th, 1936 (p. 310), DR. H. J. PARISH, of the Wellcome Laboratories, contributes a note giving data of 14 cases (not included above) in which the Schick test gave rise to allergic symptoms; six in America and the rest, in England. DR. PARISH says that he had long suspected the occurrence of other cases, and Freedman had informed him "that several physicians in America had observed allergic reactions of varying degree following a Schick test performed some time after a previous Schick test. In most cases the symptoms appeared within a few minutes of the injection, and consisted of swelling at the sites of injection in about half the cases.
In some there was puffiness of the face, swelling in axillae, faintness, cyanosis and dyspnoea; there is also mention of swelling of the tongue, nausea, sometimes going on to vomiting and diarrhoea, pain in epigastrium and back, oppression of chest, coughing, restlessness and slight temperature. Bronchial asthma occurred in more than half the cases.
(f) The Lancet, August 15th, 1936, drew attention, in a leading article on "Reactions after Diphtheria Tests," to two rare types of reaction that may follow the Maloney and Schick tests in order, it was stated, that workers, having a clear picture of them, "will not be surprised or unduly alarmed if they meet them." (p. 389.)
(g) In a leading article on "Prophylaxis of Diphtheria" in the British Medical Journal, October 10th, 1936, we are told : —
"It is interesting that, very rarely, a patient is met with who, alter immunization, previous test, or infection with diphtheria, is sensitive to Schick toxin, and shows symptoms of allergy shortly after injection. These are generally mild, and in the very few instances of severe reaction reported the condition has been controlled with adrenaline." (p. 723.)
(h) In the Medical Officer, November 7th, 1936, Guy BOUSFIELD, M.D., B.S.Lond., of the Camberwell Research Laboratories, referred to the article in the Lancet already quoted (August 8th, 1936), and went on to give two illustrative cases from his own experience. One, a girl of six, was severe. She had been immunised with three injections of toxoid-antitoxin floccules three months previously. He wrote : —
"About 15 minutes after the test she was brought back to the clinic suffering from fairly severe cyanosis, dyspnoea and oedema of the forehead, eyelids, face, lips and neck generally. The alae nasi (nostrils) were markedly active, and there was pronounced respiratory distress." (p. 193.)
In this case, as in others, adrenalin was injected and the attack passed off in 1 1/2 hours. DR. BOUSFIELD admitted that cases have occurred with Schick tests following immunisation with four different kinds of mixtures, all of which contained toxoid.
(i) H. A. RAEBURN, M.D., M.R.C.P., D.P.H;, reported in the Lancet, September 11th, 1937, three cases of unusual reaction to the Schick test: one, developing engorged lymphatics up the arms as far as the elbow; a second, showing an indurated area at the site of injection surrounded by a ring of small haemorrhages into the skin; the third, a nurse, presenting an eruption of herpes labialis. (p. 622.)
Further evidence of the liability of even the minute quantities of foreign protein contained in the test dose to give rise to allergic disturbances will be found in Section VIII, page 86. A fatal case of anaphylactic shock following a skin-test for sensitivity to horse serum is described on page 89.
Section 5
"SCHICK" IMMUNISATION
This consists of a series of injections under the skin, at variable intervals, of the TOXIN derived from the Kiebs-Loeffler bacillus prepared in various ways, either alone or mixed with a certain quantity of antitoxic serum (from a horse or goat).
(a) Between 1913 and 1924, according to DR. ABRAHAM ZINGHER in the New York State Journal of Medicine (February, 1934), some 14 varieties of toxin-antitoxin had been in use in New York.
(b) Toxoid is toxin treated by heat and formalin to render it less dangerous. It is known as Anatoxine (Ramon) on the Continent.
(c) Because of the possibility of Toxoid reverting to Toxin, it has frequently been mixed with antitoxin, and the resulting toxoid-antitoxin mixture is the one most commonly in use in this country, according to SIR GEORGE NEWMAN’S Report in 1926, and SIR HILTON YOUNG in the House of Commons, March 15th, 1934.
(d) Alum-toxoid, toxoid-antitoxin floccules, and toxoid alum-precipitated are three further variants devised with a view to avoiding some of the more distressing reactions of their predecessors. [As the Report of the Committee of the British Medical Association on Immunisation including Vaccination (1935) stated: —the immunologist has evolved an almost bewildering multiplicity of prophylactics in his attempts to avoid reactions." (p. 12.) ]
Nevertheless, the latest Memorandum issued by the Ministry of Health (170/Med. November, 1932), gives no guidance as to the use of any particular preparation, but leaves public health authorities to order any of the substances in question through the manufacturing chemists and importers, of whom it supplies a list [See quotation from the Medical Officer. Section VII, p. 68.]
Each of the foregoing substances has been in turn declared by the manufacturers harmless and effective, but in spite of laboratory tests and assertions, a long series of tragedies has occurred in various parts of the world since 1919 [See Section VI, p. 62.]
The normal variation in the incidence of diphtheria is so great from year to year and from place to place that only statistics dealing with large numbers can be considered reliable evidence.
1. DR. J. GRAHAM FORBES, in his monograph, The Prevention of Diphtheria, published by the Medical Research Council in 1927, tells us:—
An extensive effort was set on foot in January, 1926, to eradicate diphtheria from New York State in the next five years."
Following successive years of decline both the cases and deaths increased in number, as the following figures (from the Lancet, May 18th, 1929, p. 1043), clearly show:—
Year Cases
Deaths
1926 7,530 477
1927 13,500 717
1928 10,776 642
2. The writer of the Weekly Bulletin, New York City Dept. of Health, had already commented in June, 1927:—
"I am at a loss to understand the increased mortality from this cause in view of the efforts made to toxin-antitoxinate many of the children in the city."
These efforts were fairly universal throughout the States, and the following figures, taken from the United States Public Health Service in Public Health Reports (February 10th, 1928), indicate the results: —
The total cases of Diphtheria in 37 States,
with a population of 90,000,000
in 1926 ... 68,668
in 1927 ... 80,152
3. A Report on the mortality rates in 93 cities of the United States, which is to be found in the Journal of the American Medical Association, May 26th, 1934 (p. 1758), gives tables showing the death-rates in 5-yearly periods from 1890 to 1933. These indicate that the general decline which had occurred up to 1925 was in some cases maintained, but in not a few replaced by a considerable rise, especially in 1930.
There is, at all events, no evidence here that the advent of the practice of immunisation had any consistent effect on the death-rates. Even in the Report itself the doubt is expressed whether the diminution may not be due "to the effect of a natural fluctuation in the prevalence or fatality of diphtheria." (p. 1758.)
4. DR. E. ASHWORTH UNDERWOOD, in quoting statistics from New York, Chicago, Toronto and Hamilton, which had been published with a view to showing that immunisation had reduced the incidence of diphtheria in those towns, remarked : —
"Certain criticisms can be made of these results, and I am not yet certain they can be attributed solely, or even mostly, to mass immunization." (Medical Officer, May 26th, 1934.)
5.Similar doubts were expressed by DR. CARNWATH at a meeting of the Public Health Section of the British Medical Association at Bournemouth in 1934. He was reported as saying:—
"It had been claimed that the fall in diphtheria mortality in New York had been due to wholesale immunization, but during the same period there had been a corresponding fall in London without this." (British Medical Journal, August 11th, 1934, p. 274.)
The New England Journal of Medicine (Vol. 210, No. 5, February 1st, 1934, p. 275), contained an editorial headed "The Disgrace of Diphtheria," in which it was declared that " as the Bulletin of the Metropolitan Life Insurance Co. points out, there are a number of States and large cities where the diphtheria death-rate to-day is not only disgracefully high, but actually increasing."
"Four States in 1932 registered death-rates from diphtheria in excess of 13 per 100,000. In New Mexico, which with 19.5 per 100,000 had the highest rate in the country, the 1932 figure was actually 34 per cent, higher than prevailed for the registration area of the United States ten years previously."
"Thirty-two large cities had in 1932 diphtheria mortality rates above the average of 4.5 per 100,000, Knoxville leading the list with 17.0, Dallas [where the disaster occurred in 1919; see p. 62, post] being a close second with 16.6."
"The worst regional picture is that of the four East South Central States: Kentucky, Tennessee, Alabama [which reports severe reactions from alum-toxoid; see p. 76] and Mississippi, and the diphtheria situation in Oklahoma, Arkansas and Louisiana . . . is characterised as deplorable."
7. In Quebec the death-rate from diphtheria fell from 144.6 per 100,000 in 1895 to 28.4 in 1922 and 6.5 in 1932. But immunisation was not started in Quebec until 1930.
8. According to an article in the Lancet, January 9th, 1935 (p.172):—
"Three years ago E. S. Godfrey (Amer. Jour. Pub. Health, 1932, xxii, 237) showed that the incidence of diphtheria in all of ten American towns did not fall, even after 50 per cent, or more of the school children had been immunized."
9. MR. HARRY B. ANDERSON, Secretary, Citizens’ Medical Reference Bureau, Inc., 1860, Broadway, N.Y., U.S.A., stated in a letter to the Medical Officer, dated June 27th, 1935:—
"A few facts stand out with regard to diphtheria in the United States. Only a small fraction of the decline in the death-rate from diphtheria took place after various boards of health set out to wipe it out through immunisation. More than 90 per cent. of the decline from 1875 to date for New York City, where statistics are available, took place before these campaigns were inaugurated."
10. DR. A. S. M. MACGREGOR, Medical Officer of Health for Glasgow, is reported in the Glasgow Herald, May 10th, 1937, to have stated in an interview that with regard to the claims made by one or two American communities as to a reduction in diphtheria incidence due to immunisation : —
"Even in these cases, however, the figures have been regarded as somewhat unreliable in respect that cognisance has not been taken of other factors which may have contributed to the improvement."
11. As immunisation has been more and more practised in New York the number of cases of diphtheria in immunised persons has increased. In 1936, according to the Municipal Engineering and Sanitary Record, April 8th, 1937, there were 249 cases, and this failure of immunisation has led to the suggestion that the operation will have to be renewed, possibly yearly. Periodic injections were recommended in this country by DRs. H. J. PANISH and J. WRIGHT in the Lancet, March 16th, 1935 (p. 605), even when the " subjects have been immunised with the most potent prophylactics available.
EVIDENCE FROM FRANCE
12. The Bulletin of the International Bureau of Hygiene (Supplement) for September, 1936, contained a long report showing that in spite of the 2,881,081 vaccinations against diphtheria which had been performed between 1925-1934, the diphtheria incidence of the whole country remained higher in 1934 than for any of the twenty years prior to 1927. (Yet vaccination was made compulsory in 1938; see n. 60.)
EVIDENCE FROM GERMANY
13. The Deutsche Med. Woch., Nov. 25th, 1932, reported that among 100,000 children, immunised with three injections, 102 cases of diphtheria, 3 of which were fatal, occurred "more than one month after the carrying out of the protective inoculation, therefore at a time when the immunising effect of the protective inoculation ought to be completely developed." Note: These cases occurred during a period of observation of one year only.
14. In addition to the opinion of the eminent DR. FRIEDBERGER, which is given under a subsequent heading, [See under heading: Fallacy underlying favourable reports] the following statement by J. WÜSTENBERG, a German medical scientist, quoted in the British Medical Journal, October 31st, 1936, is of particular significance : —
"Although wholesale immunisation against diphtheria has been undertaken in Germany during the past few years, opinions are yet divided about its value." (Epit. of curr. med. lit., p. 69.)
15. No doubt this division of opinion owes its origin to the fact of the extraordinary rise within recent years in both the incidence and fatality-rate of diphtheria in Germany, a country in which, it is admitted, immunisation has been carried out in a most thorough manner. The following are the figures relating to diphtheria during the period 1932 to 1936:—
| Year | Cases of Diphtheria | Fatal Cases | Fatality rate | Incidence per 100,000 living |
| 1932 | 64,138 | 2,974 | 4.6 | 99 |
| 1933 | 74,558 | 3,628 | 4.8 | 114 |
| 1934 | 114,007 | 4,807 | 4.2 | 175 |
| 1935 | 132,930 | 5,795 | 4.3 | 199 |
| 1936 | 149,971 | 5,788 | 3.9 | 224 |
The above figures show that whilst the number of cases of diphtheria in Germany has steadily increased since 1932 in proportion to the increase in population, the actual deaths have nearly doubled.
Diphtheria Mortality per 100,000 Living.
| Year | Birmingham | Leicester | Sheffield | Nottingham | Coventry | Northampton | Derby | Stoke on Trent |
| 1920 | 22 | 17 | 6 | 34 | 7 | 10 | 8 | 8 |
| 1921 | 13 | 10 | 4 | 10 | 6 | 10 | 7 | 7 |
| 1922 | 10 | 8 | 7 | 4 | - | 10 | 8 | 6 |
| 1923 | 15 | 4 | 3 | 4 | 5 | 4 | 2 | 3 |
| 1924 | 10 | 15 | 4 | 4 | 6 | 1 | 21 | 3 |
| 1925 | 10 | 14 | 6 | 9 | 11 | - | 11 | 7 |
| 1926 | 12 | 15 | 10 | 26 | 4 | 16 | 14 | 8 |
| Inoculation campaign started | Practically no inoculation in these towns |
|||||||
| 1927 | 6 | 4 | 6 | 23 | 15 | 5 | 9 | 4 |
| 1928 | 7 | 7 | 7 | 16 | 26 | 7 | 12 | 2 |
| 1929 | 9 | 5 | 7 | 21 | 21 | 13 | 11 | 4 |
| 1930 | 9 | 3 | 4 | 13 | 23 | 9 | 16 | 4 |
| 1931 | 6 | 2 | 1 | 2 | 6 | 4 | 11 | 6 |
| 1932 | 3 | 2 | 1 | 3 | 2 | 1 | 7 | 2 |
| 1933 | 3 | 4 | 4 | 2 | 6 | 1 | 6 | 2 |
| 1934 | 8 | 8 | 8 | 2 | 6 | 2 | 6 | 2 |
| 1935 | 8.2 | 3.1 | 14.2 | 5 | 6.9 | 3.1 | 13.5 | 4.7 |
| 1936 | 6.3 | 2.7 | 16.8 | 9.7 | 8.2 | 1.0 | 7.1 | 6.6 |
| 1937 | 7.9 | 7.6 | 8.3 | 2.5 | 3.4 | 5.2 | 4.3 | 11.7 |
Although DR. KILLICK MILLARD is "in no sense hostile to inoculation on principle," he comments [See section 12, par 16] :
"It will be noticed that a big drop in diphtheria mortality in Birmingham occurred the very year after the inoculation campaign was started. At this time, the number of children who had been inoculated was insignificant . . . So that the drop which occurred in the years immediately following the inoculation campaign clearly cannot be ascribed to the inoculation campaign. The further drop which occurred in the two years 1931-2, however, might well have been attributed to it, but for the fact that a precisely similar drop has occurred in other neighbouring towns—Leicester, Sheffield, Nottingham, Northampton, Coventry, etc. (See Table.)
"Up to the present, it is difficult from the Birmingham experience, if compared with that of neighbouring towns, to feel such assurance that any material results have been achieved." (Medical Officer, March 9th, 1935, p. 95.)
The figures which have become available since DR. KILLICK MILLARD’S Report lend little encouragement to the supporters of immunisation. They show that diphtheria is a disease which tends to evince rapid fluctuations in severity unrelated to any artificial measures of a preventive nature which may have been taken. Bearing in mind the statistical tricks which have been employed to secure an apparent reduction in diphtheria mortality in cities such as Birmingham [See section 9, p94] it may be instructive to compare the average mortality over a period of five years before the introduction of immunisation with that of a similar period subsequent to this: —
COMPARING DIPHTHERIA MORTALITY PER 100,000 BEFORE AND AFTER IMMUNISATION CAMPAIGN IN BIRMINGHAM.
| Birmingham | Leicester | Sheffield | Nottingham | Coventry | Northampton | Derby | Stoke on Trent | |
| A. Average of 5 years 1922-1926 | 11.4 | 11.2 | 6.0 | 9.4 | 6.5 | 8.25 | 11.2 | 5.4 |
| B. Average of 5 years 1933-37 | 6.6 | 5.1 | 10.2 | 4.24 | 5.1 | 2.46 | 7.4 | 5.4 |
| B. As % of A | 58 | 44* | 170 | 45* | 78 | 29* | 66 | 100 |
This table shows that in three towns* in which immunisation has not been carried out to any great extent, the incidence of diphtheria has fallen to an even greater extent than in Birmingham.
17. Another city in which immunisation has been extensively practised is Liverpool. A Medical Officer from the Liverpool Health Department informed the Liverpool Daily Post (February 17th, 1938), that during the last ten years upwards of 50,000 persons, chiefly children, had been inoculated and that at the present time inoculations were proceeding at the rate of about 8,000 per annum. The work had not, he said, materially influenced the general prevalence of the disease, which had been high for a number of years.
18. On the other hand, in his report on school medical work at Northampton during 1932 [See section 12, p118, par 3], DR. STEPHEN Rowland, Medical Officer of Health, in referring to the drop in diphtheria incidence in that city, suggested that there was some other factor besides the causal organism which gave rise to "long waves of disease of twenty or thirty years or more," a factor not at present understood [See section X, p. 104, also J. E. R. McD0NAGH: The Common Cold and Influenza (Heinemann, 1936), p. 79, et seq.] He added : —
"It is of interest to note this great fall in the diphtheria rate [1930:286; 1931 :83; 1932:39 notifications received] has not been brought about by Immunisation and it is easy to see that much of the decrease in diphtheria following Schick immunisation may be unconnected with this process as it is in Northampton." (Medical Officer, July 15th, 1933, p. 29.)
19. On the other band, we read in the Colne Times, January 7th, 1938:-
"In the annual report of the County Medical Officer we note that the number of notifications of diphtheria rose from 2,360 with 155 deaths in the year 1935 to 3,025 with 179 deaths in the year under report (1936). This was the greatest incidence in the County since the year 1901. Immunisation was undertaken in some 35 districts."
20. No wonder DR. T. CROWLEY, Medical Superintendent of the Wath Wood Hospital and M.O.H. for Wath-on-Dearne, is reported to have declared:—
"Where they have done most immunising they are getting the most diphtheria." (South Yorkshire Times, March 11th, 1938.)
MR. A. FOUCHARD, a member of the County Council Public Health Committee, speaking at the same meeting of the Hospital Board, confirmed the statement made by DR. CROWLEY, remarking that : —
"Where immunisation takes place the rate has gone up, because you are creating carriers in the immunised districts."
He then went on to declare : —
"In a statement I made to the Public Health Committee at County Hall—and the County Medical Officer acquiesced—you must either abolish diphtheria immunisation or make it compulsory with 100 per cent. immunisation."
This convenient explanation of the failure of immunisation has been put forward by several other authorities [see page 57, post] but the principle of the danger of carriers upon which it is based has been shown by DR. H. P. NEWSHOLME, M.O.H. for Birmingham, to be without foundation. His experience of diphtheria in eight completely immunised residential schools, representing a total of some 1,500 children, showed that the incidence of diphtheria among the new entrants, numbering some 2,200 over a period of ten years, was lower than the incidence rate among the population as a whole. He therefore concluded that the danger of carriers under such conditions could not be upheld [See the Medical Officer, April 13th, 1935, p150, see also p.8, par6]. This is another striking illustration of the confusion of contradictory statements which surrounds the whole subject; there is hardly a principle regarding immunisation and immunity upon which the leading medical authorities can agree among themselves.
21. DR. B. ASHWORTH UNDERWOOD, Deputy M.O.H. for Leeds, wrote in regard to the immunisation of children in that city that : —
"it was found that the ordinary prophylactics such as T.A.M. (toxoid-antitoxin mixture) gave results which were quite unsatisfactory." (Medical Officer, 26th May, 1934.)
This statement alone is surely remarkable seeing that DRS. FLEMING and PETRIE [See page 71, post], in Recent Advances in Vaccine and Serum Therapy (1934) had written : —"The most extensively used diphtheria prophylactic in England since 1924 has been a toxoid-antitoxin mixture." (p. 428.)
IMMUNISED PERSONS CONTRACT DIPHTHERIA.
PROFESSOR W. W. C. TOPLEY, in his book An Outline of Immunity (1933), states: —
"We should never accept the proof that active immunization will convert a Schick-positive to a Schick-negative reactor as final evidence that this procedure will protect against natural infection." (p. 329.)
1. According to the M.O.H. for Winnipeg, DR. A. J. DOUGLAS, of 268 cases of diphtheria (occuring between January 1st and November 30th, 1930), 17 had been immunised: 3 in 1925; 4 in 1926; 3 in 1927; 3 in 1928; and 4 in 1929. (Report, December 15th, 1930.)
2. According to the Winnipeg Department of Health and School Board Health Department, toxoid was introduced in 1925. In the succeeding six years:
Among 195,689 NON-immunised children there were 875 cases of diphtheria; that is, 447
per 100,000.
Among 11,259 immunised children there were 52 cases of diphtheria; that is, 461 per
100,000.
3. A letter signed " Medico " in the New York Medical Week, March 28th, 1931, reads:—
"It might be interesting to note that the majority of cases of diphtheria which I have seen during the past year has been in children who have received toxin-antitoxin at the hands of our public agencies."
4. The Journal of the American Medical Association, May 20th, 1933, reported two cases of vaccinated children developing clinical diphtheria. "Both children had been vaccinated in a perfectly proper manner, one three months and the other five months before being taken ill," (p. 1618.)
5. The Journal of the American Medical Association.. September 14th, 1935, reported that three children "who apparently had been immunised to the extent of a negative Schick test contracted diphtheria after the final test was reported negative." (p. 889.)
6. The New York State Journal of Medicine, April 15th, 1936, contained an article by JAMES E. PERKINS, M.D., Division of Communicable Diseases, New York State Department of Health, describing an outbreak of 20 cases of diphtheria, of whom 14 were nurses in an up-State New York Hospital. "In ten of the fourteen cases in which there was a history of a previous Schick test, it was claimed that the test had been negative." Ten of the twenty patients had previously received injections of toxoid or toxin-antitoxin, seven more than a month prior to onset of illness. Four cases had been passively immunised with antitoxin from 8 to 15 days before developing diphtheria.
7. The Medical Officer, October 31st, 1936 (p. 181) recorded that in ten years amongst children immunised prior to 1931 in Winnipeg there occurred 75 cases of diphtheria, with 2 deaths. In the six years 1930-35 there were 45 cases, with 1 death among immunised children.
8. The Municipal Engineering and Sanitary Record, April 8th, 1937, reported that an investigation made by the Health Department of New York, revealed that out of 668 cases of diphtheria in children under 15 as many as 249 had received immunising injections.
9. The British Medical Journal, April 13th, 1935 (Epit. of curr. med. lit.) reported the observations of C. J. BRENKMAN, G. H. DE JONG, M. G. NEURDENBURG, H. PETERS and H. W. HOESEN regarding active immunisation by toxin-antitoxin in Amsterdam and Rotterdam (1928-30). In Amsterdam 91.2 per
1,000 of children of 14 years and under were immunised, of whom 4.3 per 1,000 subsequently contracted diphtheria; in Rotterdam 146 per 1,000 were immunised and of these 10.5 per 1,000 subsequently contracted diphtheria. (p. 59.)
EVIDENCE FROM ENGLAND AND WALES
In DR. J. GRAHAM FORBES’ book on Diphtheria; its Distribution and Prevention, there are reports of at least 330 cases of diphtheria that developed two months or more after the final inoculation.
Birmingham.
10. DR. G. A. AUDEN, School Medical Officer for Birmingham, admitted in the Medical
Officer (p. 201), May 16th, 1936, that 36 cases of diphtheria had occurred in fully
immunised children during the previous ten years.
11. It must also be borne in mind that in reply to a question in the House of Commons on March 19th, 1935, the Minister of Health stated that between 1931 and 1933, 30 cases in Birmingham sent to hospital as diphtheria, in which the patient had been previously immunised, had been re-diagnosed as tonsillitis. (See p. 94, post.)
12. According to a letter received from the Minister of Health in answer to a question in the House of Commons and dated March 30th, 1938, 81 children under 15 years of age in Birmingham who had been inoculated against diphtheria have contracted diphtheria since the introduction of inoculalion in 1925.
Bristol.
13. The M.O.H. for Bristol, DR. DAVIES, in the Lancet, November 21st, 1931,
reported 44 children who developed diphtheria after having been fully immunised with three
injections. Five of them had been "proved" to be immune by the Schick test. Nine
were virulent, and one of them died 85 days after the third injection. He confesses:
—
"It is disconcerting to find cases of clinical diphtheria occurring in Schick-negative children and at such periods after the course. The periods varied from 185 to 204 days." (p. 1153.)
Cardiff
14. In reply to a question in the House of Commons on July 10th, 1937, the Minister of
Health stated that up to the end of 1936, 195 immunised children under 15 years in Cardiff
had contracted diphtheria.
Dewsbury
15.On June 20th, 1934, MR. GROVES asked the Minister of Health how many cases of
diphtheria and deaths from that disease have occurred in Dewsbury in immunised children
since immunisation was first started in that town; and how many months had elapsed since
the last inoculation before diphtheria developed in these cases?
SIR H. YOUNG: The following is the information furnished by the local authority on this subject.
The number of cases of diphtheria and deaths therefrom occurring in "immunised" children was as follows : —
1932 1933 1934
(January 1st to June 13th)
Cases 13 26 23
Deaths 4 2
3
The following table, summarised from Sir Hilton Young’s figures, shows the number of cases which occurred within six months of the last injection and those which occurred between the seventh and twenty-first month respectively, the latter being indisputably cases of diphtheria in fully immunised children.
Months since last injection 1932 1933 1934
lst to 6th ... ...
13 6 2
7th to 21st ... ...
nil 20 21
It will be noted that even allowing for the full six months’ interval since the last injection (which is claimed by some as the period necessary for immunity to develop) this table alone reveals 41 cases of diphtheria in fully "immunised" children. A question in the House of Commons on February 25th, 1935, elicited from the Minister of Health the fact that in 1934, in addition to the above, four cases, with two deaths, from diphtheria occurred in children who had been immunised at least 10 months previously. On March 15th, 1935, a question to the Minister of Health elicited the fact that all 11 deaths occurred in children who had been inoculated at least three months prior to infection.
Folkestone
16. DR. AUSTIN PRIESTMAN, Medical Officer for Folkestone, reported in the Medical
Officer, March 9th, 1935, his unfavourable experiences with diphtheria immunisation as
follows:—
"The active immunisation of two groups of children, one a visiting group of campers and another a group in a local institution, would have ruined my advocacy in the eyes of the Council. "Both these groups, some months after immunisation, when it should have been effective, developed clinical diphtheria with organisms of a virulent type, typical myocardial weakness, etc." (p. 99.)
His conclusions as to better methods of prevention are given on page 109, post.
Hackney
17. In answer to a question in the House of Commons on July 18th, 1935, the Minister of
Health stated that five children in Hackney, who had received the full prescribed course
of injections, had contracted diphtheria since the practice was introduced into the
Borough.
Huddersfield
18. In answer to a question in the House of Commons, the Minister of Health wrote on July
22nd, 1988, that during the five years 1933-37, 44 cases of diphtheria were notified in
Huddersfield among immunised children, of whom one died.
Leeds
19. In the Lancet, February 16th, 1935, ASHWORTH UNDERWOOD, B.Sc., M.B., D.P.H.,
Medical Officer of Health for Shoreditch and late Deputy M.O.H. for Leeds, discussed 20
cases of diphtheria at Leeds which " had been definitely immune acording to accepted
standards, at some time before, or actually at the onset of disease." Eighteen of
these cases were persons who had been inoculated against diphtheria, and had subsequently
been pronounced Schick-negative. Sixteen of these cases were definitely diagnosed as
"clinical diphtheria," and the other four were sub-clinical. Eight cases, which
were shown to be Schick-negative at the time of infection, were" so severe that in
every case except one 16,000 units or more of anti-serum were considered necessary for
treatment." (p. 366.)
On April 6th, 1938, the Minister of Health informed Mr. Tom Groves, J.P., M.P., that during the years 1933 to 1937, 201 immunised children and 3 immunised adults had subsequently contracted diphtheria.
Leicester
20. According to the Medical Officer, October 8th, 1938, DR. E. K. MACDONALD,
Medical Officer of Health for Leicester, reported that during the year 1937, among the
3,000 children immunised there had been six cases of diphtheria.
The Editor commented as follows: —
"It is now generally conceded that immunisation is not an absolute protection against any assault of corynebacterium at any time, but it raises resistance to a point almost proof against the strains of lesser virulence and reduces the danger from the severer strains so that the latter, if they produce any reaction at all, do not produce serious lesions." (p. 155.)
So that it is admitted that at best immunisation can only be counted upon when it is least needed—when the infection is a mild one. As to the second part of the claim, evidence that it has no effect upon the severity of attack will be found on page 55.
Liverpool
21. In reply to a question in the House of Commons the Minister of Health, on August 1st,
1935, stated that out of 19,504 children under 10 years in Liverpool who had been
inoculated between 1928 and 1934, 60 had developed diphtheria and of these 4 had proved
fatal.
22. In reply to a question in the House the Minister of Health wrote (April 6th, 1938), that between 1933 and 1937, 201 immunised children and 3 adults had contracted diphtheria. Of the cases (3 over 15 years of age) which occurred between 1935 and 1937, 12 had developed the disease within 3 to 6 months of the inoculation, and 176 more than 6 months after inoculation. Six of the latter cases were fatal.
From these figures it follows that between 1928 and 1937 in Liverpool, there have occurred 248 cases of diphtheria with 10 deaths in inoculated persons, all but three of whom were under 15 years of age, and all of whom became infected after an interval of three months from the time of inoculation.
Manchester
23. DR. R. VEITCH CLARK, Medical Officer of Health for Manchester, in a report to the
City Council on July 7th, 1937, admitted 100 cases of diphtheria had occurred among a
selected immunised class of children.
24. In reply to a question in the House on April 21st, 1938, the Minister of Health admitted that in Manchester from 1927, when immunisation started, until the end of 1937, there had been 149 cases of diphtheria, including three deaths, in inoculated persons; in addition, there had been a fatal case in a known Schick-negative child.
Poole
25. In reply to a question in the House of Commons on February 9th, 1937, the Minister of
Health stated that five children in Poole, who had received one or more inoculations
against diphtheria, had been notified as suffering from the disease.
Southampton
26. H. C. MAURICE WILLIAMS, M.R.C.S., L.R.C.P., D.P.H., Medical Officer of Health for
Southampton, J. D. DEAR, M.B., Ch.B.(Edin.), D.P.H., Senior Assistant M.O., and W. STUART,
M.B., Ch.B.(Aberd.), D.P.H., Assistant School M.O., writing in the British Medical
Journal; November 28th, 1936 (p. 1078), on the relative values of "one-shot"
alum-precipitated toxoid and three injections of toxoid antitoxin mixtures, come to the
conclusion that "severe diphtheria is possible after either method of
immunisation." They stated that out of 1,180 children under 16 notified as diphtheria
cases between June, 1934, and May, 1936, 44, or 3.7 per cent., had been immunised or found
to be immune. Three of the former were severe.
Wakefield
27. In reply to a question in the House of Commons the Minister of Health wrote (July 2nd,
1938), that 123 cases of diphtheria had been notified in Wakefield among patients who had
attended the immunisation clinic since it opened.
Wood Green
28. In his Annual Report for 1936, DR. MALCOLM MANSON, M.O.H. for Wood Green,
stated that, in an outbreak of diphtheria in the borough, out of 56 cases "eight had
been immunised, and of these seven had been post-Schicked and found to be negative."
Dr. Manson admits his disappointment.
29. In the Brit. Med. Jour. (Epit. of curr. med. lit., p. 92), of December 2nd, 1933, we may read : —
"M. Fayot (These de Paris, 1933, No. 487), who records 130 cases in patients aged from 14 months to 14 years in which diphtheria had occurred in spite of injections of anatoxin (toxoid), states that diphtheria in the inoculated occurs in about 3.3 per cent, of all the cases of diphtheria and has been noted in 11.6 per cent. of the cases at the Hopital des Enfants Malades in Paris in recent years."
30. The Deutsche Med. Woch., Nov. 25th, 1932 (p. 1885), reported: —
"There are persons in whom also a triple anatoxin inoculation is unable to produce even a slight degree of immunity." (See p. 43, par. 13.)
31. The experience of W. REINHARDT, reported in the Deutsche Medizinische Wochenschrift (April 8th, 1938, p. 535), is summarised in the British Medical Journal, June 25th, 1938 (Epit. of curr. med. lit., p. 108), as follows:—
"In a convalescent home, housing on an average 110 children, as many as sixteen cases of diphtheria occurred, although the children had been actively immunised at a time when there was no epidemic of diphtheria. All the children had been examined for diphtheria bacilli in the nose and throat before being admitted to this home, and the bacteriological reports had been consistently negative. The children had, in fact, been artificially immunised against diphtheria under the best conditions. The shortest interval between immunisation and the outbreak of the disease was one of seventeen days, and in four cases this interval was longer than three months. The behaviour of the diphtheria in these sixteen cases was what might be expected in children not immunised; the disease ran a light course in four cases, a moderately severe course in ten cases, and a severe course in two. In a footnote to his article the author states that twelve further cases of diphtheria have recently broken out in the same convalescent home among children who had been artificially immunised; the interval between immunisation and the outbreak of the disease had ranged from one to three months in most cases, but had twice been less than twenty days and had once been almost nine months. The author contrasts these observations with the claims made on behalf of active diphtheria immunisation that the immunity it confers begins in four to five weeks and lasts several years [In Therapeutic Notes. January, 1935, it is stated: "Active immunity lasts for several years, if, indeed, not for life." (p. 17.)]. The principle of such immunisation is not challenged by him but he does insist that there is evidently room for improvement in the technique."
County Cork
32. The M.O.H. for Cork, reporting on a "campaign of active immunisation . . . in
which toxoid antitoxin was the prophylactic used," remarks that: —
"The success of the effort was greatly hampered by the continual occurrence of reported cases of diphtheria among treated or partially-treated children. It was in an attempt to prevent such cases that alum toxoid was introduced." (The Lancet, April 15th, 1933, p. 795.)
County Galway
83. DR. C. H. FOLEY, Athenry, Co. Galway, reported in the British Medical Journal, April
13th, 1935, "a case of diphtheria of virulent form in a school child who had had
three injections of T.A.M. in the previous Sepember," he having been called to the
case on Christmas Day. " In the next two days a second child in that cottage, who had
also received three injections of T.A.M. in September, developed diphtheria." Later
he met with three other similar cases. He added: "Here is a country school in a
healthy rural district, with a small average, say fifty children, all immunized with three
injections of T.A.M., yet at least five, if not more, develop not mild but severe
diphtheria. Does it matter really what we say when the public judges treatment by
results." (p. 812.)
34. In the Bulletin of Hygiene, March, 1933, the following comment appears in the section dealing with " Infective Diseases ":
"It is pointed out that in Rome, where 28,340 children were immunized in the three years 1929-31, both the morbidity and mortality-rates from diphtheria have slightly increased rather than decreased during the period."
Aberdeen
35. In reply to a question in the House of Commons on July 28th, 1938, the Secretary of
State for Scotland stated that in Aberdeen 23 immunised children had suffered from
diphtheria since September, 1936.
Edinburgh
36. In reply to a question in the House of Commons on July 28th, 1988, the Secretary of
State for Scotland stated that out of approximately 27,000 children in Edinburgh, who had
been inoculated against diphtheria since 1924, 140 had contracted diphtheria, and of these
three had proved fatal.
Glasgow
37. DR. A. S. M. MACGREGOR, Medical Officer of Health for Glasgow, was reported in the Glasgow
Herald, May 10th, 1937, as saying that although there had been no organised public
system of immunisation in the city, statistics of health progress showed that Glasgow was
not suffering from so high an incidence of diptheria as Aberdeen and Edinburgh, where
immunisation had been pushed for many years. In 1934 the diphtheria death rate per million
inhabitants was 144; in 1935 it was 102, and in 1936 came down to 48.
In the light of the foregoing evidence it is manifestly absurd for statements to be made implying that the protection afforded by inoculation is complete, such as the following typical one by the M.O.H. for Beckenham : —
"Diphtheria can be regarded as an ‘optional disease,’ as far as the individual is concerned." (Annual Report for 1928.)
IMMUNISATION HAS NO EFFECT ON SEVERITY OF ATTACK.
1. It is frequently asserted that diphtheria is less fatal in the inoculated [In a booklet issued in 1936 by the L.C.C., entitled "Nomenclature of Diptheria Infections", it is stated that "such cases are uncommon and invariably mild." (p9)]. In the Brit. Med. Jour. (Epit. of curr. med. lit., p. 92) a statement of M. Fayot’s is quoted (These de Paris, 1933, No.487), that it has been observed in France that: "Diphtheria following inoculation does not present any special features. It may -be severe and even fatal . . ." (See p. 52, par. 26, and p. 53, par. 31.)
2. D. T. ROBINSON, M.Sc., M.R.C.S., and F. N. MARSHALL, M.D., D.P.H., in an article in the Lancet, August 24th, 1935 (p. 444) confessed that: —
"The claim, often made in the past, that clinical infection in Schick-negatives is always mild can obviously no longer be upheld—certainly not in areas where the gravis strain abounds."
On the same page they give a table of eleven cases of diphtheria which had received three 1 c.cm. injections of toxoid-antitoxin mixture (T.A.M.) at least six months previously. Only one of these cases was mild, and one actually died.
3. DR. A. E. PLATT, of Adelaide University, writing in the South Australian Public Health Notes, July, 1937, confessed:
"During an outbreak of diphtheria at Quorn four cases were reported where children who had been immunised many months before contracted the disease and in three the germ strains were of the gravis type" (i.e., severe; actually three of the cases died).
"In February, 1936, Gregory reported this type in Victoria, and about the same time it was observed in New South Wales. "Where diphtheria has appeared in immunised persons the gravis type has almost always been the one concerned."
FALLACY UNDERLYING DESCRIPTION "MILD."
Moreover, recent scientific observation has established that what is frequently described as "mild" diphtheria may be followed by serious consequences.
1. In the Medical World, March 1st, 1935, DR. ELWIN NASH, M.O.H. for Heston and Isleworth, explained that it is little use ensuring that a child "has a mild attack of diphtheria, as no one can foresee what the outcome is going to be in the matter of cardiac or renal complications in a case which at the commencement may appear to be slight."
2. In the Epitome of Current Medical Literature in the British )~iedical Journal, August 22nd, 1936, is a summary of an article by W. BEHR in the Deut. Med. Woch. (May 8th, 1936, p. 771), in which it is stated that occasionally an apparently mild diphtheria, treated early and effectively, was followed by the most severe paralysis. An example of this was afforded by a 5-year-old child, for whose apparently mild diphtheria 10,000 units of serum had been given on the second day; yet death occurred on the fifty-third day from respiratory paralysis.
3. The argument is also frequently heard that the "mildness" of diphtheria in the immunised is shown by the curtailment of their detention in hospital. The Medical Officer, April 4th, 1935, knocked the bottom out of this argument in unambiguous terms. "As evidence," wrote the Editor, " it is quite worthless, because length of stay depends upon the views of individuals." (p. 132.)
FALLACY UNDERLYING FAVOURABLE REPORTS.
In addition to the foregoing positive evidence of the failure of inoculation to immunise, there remain to be considered the fallacies which afford an explanation of apparently favourable statistics. These are fully dealt with in Section 9 (see p. 94).
One of the chief fallacies giving rise to erroneous conclusions was indicated by DR. FRIEDBERGER in the course of his address to the Berlin Medical Society in 1931, in the course of which he maintained that —"As regards active immunisation against diphtheria . . . its introduction had not caused any change in the occurrence of epidemics, and that all the statistics as to its success, which mainly emanated from American sources, were based on the erroneous conclusion that the decline in the incidence of diphtheria was due to immunisation, whereas the immunisation was being carried out when the disease was already showing a tendency to abate." (The Lancet, March 14th, 1981, p. 598.)
PROFESSOR W. W. C. TOPLEY writes in his book, An Outlin eof Immunity (1933) : —
‘We are here faced with a problem of great statistical difficulty. It will not do to cite a few instances in which the inauguration of mass immunization has been associated with a decline in the general diphtheria morbidity rate, because we know quite well that most infective diseases are subject to secular trends in frequency, and a falling rate for any one of them might well have no significant association with any particular preventive measure adopted at the time the fall occurred."
In an article entitled "Trends in the Prevalence of Diphtheria," which appeared in the Journal of Infectious Diseases (Chicago), Vol. 58, 1936, ESCHSCHOLTZIA L. LUCIA and HILDA F. WELKE, of the Department of Hygiene, University of California, and the Department of Public Health, San Francisco, California, discussing the difficulty of presenting evidence in favour of active immunisation [ See further quotation on p. 99.], declared : —
"The common tendency to a lowered mortality or morbidity seems to be best explained on the basis of the cyclic periodicity of the disease." (p. 307.)
GROWING SUSPICION OF "SOMETHING WRONG" WITH THE METHODS.
D.M. CAMERON, M.B., Ch.B., writing in the Pharmaceutical Journal, February 2nd, 1935, warned his readers : —
"That there is something wrong somewhere in serum and vaccine therapy is, I should think, generally agreed. Scarlet fever and diphtheria are questionable as regards the value of prophylaxis, and reactions are not sufficiently regarded by enthusiasts. Before the country is stampeded into mass immunisation this problem of side effects should be most thoroughly gone into, e.g., anaphylaxis with serum, encephalitis with vaccination." (p. 117.)
In fact, so far from immunisation proving a blessing, there is an increasing weight of opinion among medical officers that under most practical conditions its attempt may constitute a danger to public health.
In a Special Report of the Medical Research Council (No. 195; 1934) entitled "Active Immunization Against Diphtheria: Its Effect on the Distribution of Antitoxic Immunity and Case and Carrier Infection," the compilers state, as a result of 12 years’ continuous study of the problem in a semi-isolated community (Greenwich Hospital School), they have come to the conclusion that: —
"active immunisation was liable to increase the number of carriers [See A. FOUCHARD, page 46, ante. Cf. p. 8, par. 6.] of virulent bacilli and would be likely to increase diphtheria among the unprotected members of a community."
DR. C. V. DINGLE, Medical Officer for Middlesbrough, reported the Health Committee of that town that he could not advise em to go in for wholesale immunisation because:—
"Unless you can get all the children in the town done you would be no better off, because iminunisation has another effect—it causes a larger number of ’carriers’ and may do more harm than good unless everybody is protected."
"I can only say it is very good for the individual child, but it is not as good for using in the protection of a large community." (Yorkshire Post, January 16th, 1935.)
That immunisation may also lead to the appearance of a more severe type of diphtheria is revealed in a warning by DR. E. ANGUS JOHNSON, M.O.H. for Adelaide, S. Australia, which was published in the West Australasian, July 24th, 1937; it read as follows: —
"Adelaide, July 23.—An inference that immunisation against diphtheria under existing conditions may lead to an increase in the diphtheria death-rate is contained in a report on Immunisation which the city medical officer of health (Dr. E. Angus Johnson) has submitted to the city council.
He draws attention to the ‘grave’ findings of a Government investigator into the recent diphtheria outbreak at Quorn, where three patients had developed the gravis and one the intermediate strains which gave rise to a more severe form of diphtheria.
These patients were supposedly immunised from diphtheria, Dr. Johnson stated, and, as far as it was known, they were the first cases of the gravis type reported in South Australia.
Dr. Johnson says that he was, therefore, still of the opinion that the Adelaide local board of health should not recommend, for the present at any rate, general immunisation, as a lot had yet to be learnt concerning immunising and its effect on the community in general."
In what other respects the practice of injecting the various immunising materials into healthy children may have results adverse to the health of the community is a subject which receives detailed treatment in the following three sections. This section may fitly include the warning uttered in its editorial by the Medical Tunes, November, 1937:-
"We believe this is the only medical journal that has warned its readers against the risks attending immunisation against disease. To-day we have prophylactic sera or vaccines against such diseases as the common cold, influenza, typhoid, and so on. Immunisation against diphtheria is one of the latest, we might almost say one of the latest crazes. At any rate, we again wish to sound a note of warning against it. We really know far too little about the actual results of immunisation to warrant us meantime in adopting such measures. Unfortunately deaths following immunisation have been reported from time to time. This should make us go very cautiously."
SPECIAL DANGER TO INOCULATED CHILD WHO DOES NOT BECOME IMMUNE.
In an article in the Medical Officer. September 14th, 1935, DR. ELWIN H. T. NASH, Medical Officer of Health, Borough of Heston and Isleworth, and DR. Guy BOUSFIELD, Medical Officer to the Immunisation Clinic in the same borough, pointed out : —
"It must be remembered that a non-immune child, believed to be immune, is in greater danger than if it had never been taken by its parents to be protected, because there is liable to be delay in calling for medical assistance. Hence the vital importance of making certain that immunity has been established, or of warning the parents of the true position." (Italics in original.)
Since a footnote to the article states that "no quotation from the last paragraph is to be published or copied unless it contains the whole of that paragraph and the preceding one," the authors’ wishes will be respected and the paragraph which preceded the one already quoted given in full.
It certainly does not detract from the reality of the danger to which attention has been directed; in fact, it rather tends to emphasise the uncertainty which surrounds the whole procedure of immunisation. It reads as follows: —
"The difficulty of the general practitioner is that if he neglects the Schick test, he remains unwarned of pseudo-reactors, who definitely are more likely to show reaction to immunising materials of all descriptions. Obviously, also he has no idea whether he is immunising without need [NOTE: In Kensington, in 1934, it was proposed to dispense with a routine preliminary Schick test on the principle that the reaction is positive in practically every child under five and that the majority of children under twelve as susceptible; thus exposing them to both disadvantages first mentioned.] On the other hand, if he dispenses with the posterior Schick test, he must warn parents that the routine with T.A.M. may leave a proportion of children incompletely immunised [The Schick test is not used on inoculated children in Birmingham; thus exposing them to the danger mentioned last in this paragraph and also to that in the paragraph first quoted. In Lincolnshire the Council decided to dispense with the Schick test altogether, except for Sample testing in the 1 to 14 years group. Other Councils in various parts of the country may have adopted similar practices regarding the Schick test, but exact information is lacking on this point. That there has been a tendency to abandon the test in America will be seen on referring to quotations from American sources on page 28, ante.]Some children may require extra injections." (p. 111.)
That compulsory immunisation should have its advocates is surely to be deplored in view, not only of the confusion which has been shown to surround the whole subject, but of the numerous disasters which have been a tragic accompaniment of the practice ever since it was introduced and are briefly described in the next section. DR. C. C. OKELL’s statement [The article by C. C. OKELL,, M.C., M.A., &.D., F.R.c.p.; appeared in the Lancet, January 1st, 1938, deserves quotation in full did space permit. Extracts will be found in Section VI (pages 62 and 66), and in Section XII (page 124).] that" the risk of accidents must remain one of the snags in all forms of immunisation," should in itself be sufficient indication of the folly, if not criminality, of attempting to force immnunisation upon an unwilling, because enlightened, public. (See Medical World warning, p. 79, post.)
Commenting upon the advocacy of compulsory immunisation by DR. H. E. MARSDEN in the Medical Officer on January 29th, 1938, the Medical Times, March, 1938, declared:-
"With the above recommendation we entirely disagree. We now know that diphtheria, like smallpox vaccination is not altogether free from risks. Dr. Marsden’s suggestion is, therefore, a most unwise one, and ought to receive no support from at least the more far-seeing members of the medical profession."
When the Guernsey States, at the instigation of fourteen local medical men, approved in July, 1938, a law to enforce immunisation against diphtheria, a memorial [Copies of this Memorial containing the reasons of objection and a list of the names of the signatories may be obtained from the National Anti-Vaccination League, 25, Denison House, 296, Vauxhall Bridge Road, London, S.W.1. Immunisation is now compulsory in Guernsey], to the Privy Council asking that body to refuse consent to the legislation was signed by no fewer than 59 doctors, 58 of whom were registered medical men and women, and the other a doctor of philosophy.
The following items of information are published with no further comment save to remind the reader that it is on the Continent that most of the serious accidents accompanying immunisation have occurred, and that, according to DR. J. MENTON’S statement in the British Medical Journal of August 10th, 1935, they still arise [see page 70, par.9]
1. The Times (London), January 1st, 1938, published the following: —
"The Hungarian Minister of the Interior has issued regulations making inoculation against diphtheria compulsory from to-day. Hungary is said to be the first country to enforce compulsory inoculation, although in Italy partial compulsion has been in effect for some time.
2. According to the Journal Officiel de Ia République Française, June 28th, 1938, the Senate and Chamber of Deputies adopted the following law:—
"Anti-diphtheritic vaccination with an anatoxin is obligatory during the second or third year of life. Parents or guardians are held personally responsible for carrying out the said measure of which proof must be furnished at the time of admission to any school, crèche, holiday establishment, or other assembly of children."
SECTION 6
THE DANGERS OF "SCHICK" IMMUNISATION
A SERIES OF DISASTERS
A SERIES OF DISASTERS 1919-1938
The following is a list of such " Schick " inoculation disasters as have been officially reported; they undoubtedly represent but a small proportion of the accidents that have occurred all over the world in connection with the practice, but should prove more than sufficient to justify the warning of the Medical Times which was quoted towards the end of the previous section (p. 58). In this connection the words of C. C. OKELL, M.C., M.A., Sc.D., F.R.C.P., late bacteriologist to University College Hospital, are particularly significant. Writing under the caption "Grains and Scruples" in the Lancet, January 1st, 1988, he said:
"On the whole diphtheria immunisation has proved a fairly safe affair, but suppose we included in our propaganda a candid account of the various untoward accidents which have accompanied the procedure . . . If we baldly told the whole truth it is doubtful whether the public would submit to immunisation. . . . Accidents and mistakes must inevitably happen and when they take place what might have been a highly instructive lesson is usually suppressed or distorted out of recognition. Those who have had to take notice of the immunisation accidents of the past few years know that to get the truth of what really went wrong generally calls for the resources of something like a secret service. And if the technical experts have often been furtive and disingenuous in their methods the public in its turn is unfair and vindictive." (p. 48.)
1. In 1919, at Dallas, Texas, U.S.A., ten children were killed and sixty others made seriously ill by toxin-antitoxin which had passed the tests of the New York State Health Department. The Mulford Company, at Philadelphia, the manufacturers, paid damages in every case.
2. In 1924, twenty-five children in Bridgewater and twenty in Concord, U.S.A., were poisoned by toxin-antitoxin. Many had high fevers, and their arms turned black and swelled to two or three times their normal size.
3. In 1924 (September) of 40 children immunised with toxin-antitoxin in a home for infants at Baden, near Vienna, six died and a number suffered from skin necroses of various sizes at the site of the injection.
The mixture had been tested on guinea-pigs and declared non-toxic. As the result of an investigation Prof. von Pirquet advised the Austrian Ministry of Health to stop the inoculations, and for a time the practice was forbidden in Austria.
4. In 1928, the Lancet of February 4th (p. 249), refers to "a more recent Russian disaster " (Bull. Hygiene, August 1927, p. 667) in which " 14 children received toxin in place of anatoxin (i.e., toxoid); eight of them died within two weeks, four of polyneuritis within a month and two recovered after symptoms of general intoxication."
5. In 1927 also there were five deaths in immunised children in China, thirty-seven others being made seriously ill.
6. In 1928, at Bundaberg, Australia, twelve children out of seventeen who were inoculated with toxin-antitoxin died, the five others being critically ill for some time. The material had been issued and declared safe by the Public Health Department of Queensland.
The Government Medical Officer, after making post-mortem enquiry, stated as the only explanation " that latent properties in the serum suddenly became active and turned it into a virulent poison." Several families were wiped out, and " the tiny victims spent a night of intense suffering."
7. In 1930, at Medellin, Columbia, South America, forty-eight children were inoculated, with the result that many were taken ill during the same night, one died the following afternoon, fourteen others within sixty hours and two more within six weeks—a total of sixteen deaths.
According to the report in the Lancet of October 24th, 1931 (p. 923), this disaster was due to toxin being given at the third injection instead of toxoid. The symptoms recorded were:
"Extreme restlessness, convulsions, fever, diarrhoea, vomiting and severe pain at the site of the injection." Almost the whole of the 48 children were ill for three or four weeks, " fever and convulsions being common."
8. In 1932, at Charolles, in France, 172 children were immunised with anatoxin (toxoid). All were taken ill soon afterwards, developing local abscesses with abundant suppuration, necessitating surgical intervention in several cases. In one case the child died. The parents of the children demanded an official enquiry, but no explanation of the tragedy has so far been forthcoming.
It is significant that only a month before this disaster the Paris Med., November 12th, 1932, declared of anatoxin (toxoid), that it is devoid of toxicity."
9. In 1933 (April) a number of children in Italy were immunised with a single injection of an anatoxin mixture.
In the province of Chiavari over 80 inoculated children were gravely affected, some being paralysed in arms and legs, others having their sight injured. One child died. In Venice and Rovigo severe symptoms, including paralysis, supervened and death occurred in ten cases.
The Italian Government ordered the entire stoppage of diphtheria immunisation; and the National Serotherapeutic Institute at Naples, which supplied and tested the material, was, according to Press reports, closed, and the director and his assistant arrested.
10. The San Francisco News, February 16th, 1935, reported under the heading "Five Given Poison for Vaccine," that five children, who were supposed to have received an injection to immunise them against diphtheria, were found to have been given by mistake a poisonous diphtheria toxin kept in the laboratory for the purpose of animal experimentation.
According to the Health Officer the bottle was correctly labelled, but the hospital interne misread it as a result ‘The next day the five developed severe symptoms, fever, swelling of their arms with unusual pain." Two of the children, Louis Bowden, aged six, and Natalie Rojnovsky, aged five, died. The doctor was " completely exonerated."
11. In the Medical Officer, September 21st, 1935, the bare statement is made (p. 117) that " Deaths from serum shock have been recorded following a first immunisation injection; none has so far been recorded in subsequent injections, either for immunisation or for treatment."[If this statement refers to treatment by serum for subsequent infection it is obviously incorrect. Fatalities due to anaphylaxis following the injection of serum in immunised persons are described in Section VIII, p. 83 et seq.] The use of the term " serum shock " must indicate that the immunising material consisted of a mixture containing antitoxin; but no further details are given in the editorial quoted.
12. The following is a translation from Le Progrès de Saône et Loire, Rue du Temple, Châlon-sur-Saône, July 24th, 1936 :
"BRANGES. Unfortunate Results of Vaccination .—On 20th May last the third session for collective anti-diphtheritic vaccination with anatoxin from the Pasteur Laboratory was held and 124 children were submitted to it.
After the first two sessions no accident had been reported. But after the session of the 20th May, in some children intense fever was reported sometimes with vomiting eruptions and blotches.
One of them age 23 months died next day and in the day that followed the number of sick children increased 75 of them at least were attacked at the point of injection with abscesses, more or less large, certain of which, at the present moment have not yet healed. The Office of the Public Prosecutor of Châlon has laid information against X . . . . with which M. Gresset, resident judge at Louhans, is charged."
13. In the British Medical Journal, June 5th, 1937 (p. 1182) will be found an account of the death of a Waterford girl, aged 12, and the illness of 23 other children, tuberculosis having developed following the inoculation of Toxoid Antitoxin Floccules. It appears that in November 1936 the consulting physician to Ring Irish College Co Waterford, DR DANIEL T MCCARTHY, inoculated 38 children of the College with material obtained from the County Medical Officer of Health This material was TAF, "for which the makers claim a high immunising effect with a very low tendency to cause reaction."
Early in the following January the little girl, who eventually died, was taken to DR. MCCARTHY because of a circular discharging ulcer which had developed at the site of injection. By April she was much worse, consultants were called in, including the county pathologist, but in spite of their efforts she died on the 20th of the month.
What has since happened to the other 28 tuberculous cases is not known to me. So far we have been assured they will recover.
At the inquest, held on June 12th, 1937, the verdict of the jury was as follows: —
"That we unanimously agree with the medical testimony that Siobhain Ni Chionnfaolaidh died at Knockanpower, Ring, on 20th April, 1937, from toxemia and purpuric haemorrhage consequent to general miliary tuberculosis infection, and that we are of the opinion, according to the evidence placed before us, that the tuberculous condition was originated by the inoculation of prophylactic into the right arm of Siobhain Ni Chionnfaolaidh in November, 1936, and that we are of the opinion that the contents of one 25 c.c. bottle of prophylactic, labelled T.A.F. Burroughs Wellcome,’ from which a portion of the material was extracted by DR. DANIEL MCCARTHY for the purpose of the aforesaid inoculation contained tubercle bacilli, [This was emphatically denied in the Memorandum of the Ministry of Health (June, 1937), which stated that after Investigation it had been shown that the mixture used contained no tubercle bacilli; nor was it possible for there to have been substitution or subsequent introduction of bacilli. This Memorandum will be found quoted in the Vaccination Inquirer, August 2nd, 1937, pp. 135-6.] and that the inoculation was carried out by DR. MCCARTHY according to the most approved surgical technique. Every precaution was taken by him and those who assisted him to guard against infection arising from contaminated appliances and we exonerate them from any blame in this matter."
Of particular importance was the failure of an action at law brought by the father in February, 1939, against the medical officer who gave the injection and the Wellcome Foundation, Ltd., the chemists who manufactured and supplied the material, and claiming damages in respect of the death of his child and the illness of her two brothers.
It was brought out in evidence at the hearing before the President of the High Court, Dublin, and established by the verdict of the jury, that the medical officer was entirely free from blame, that nothing he did could have caused the infection, and that the elaborate precautions taken by the defendant firm of chemists precluded the possibility of any contamination of the T.A.F. supplied.
We are forced to the conclusion, therefore, that in this case, at any rate, the entire blame for illness and death must be ascribed to some properties inherent in the immunising material itself; also that such dangers are inseparable from the use of these preparations and cannot be avoided by the most scrupulous care both in manufacture and administration.
Evidence that both Toxoid-Antitoxin Floccules and Toxoid have been known to light up dormant tuberculosis will be found in the next section [see page 74 post]
That this might afford a possible explanation of the tragedy does not appear to have occurred to anyone either at the inquest or at the trial, and so far as any official pronouncement on the cause is concerned the case remains wrapped in mystery.
14. According to the Toronto Daily Star, October 29th, 1938, a nine-year-old boy named Basil Forest, who was a pupil at the Waterford district school, was inoculated, along with twenty-nine others at the school. Eleven of them were ill following the inoculation and Basil Forest himself died in Olds hospital on October 2nd, 1938, following, according to the account of the inquest, an operation on his infected arm. No reason is given as to why the inoculation should have proved fatal.
Since in many of the above disasters, after investigation, it was alleged that some mistake had been made either in manufacture or administration, they have been described separately.
At the same time, it must be pointed out that the explanations offered cannot be regarded as satisfactory, since it is difficult to understand why, if no fault lay with the immunising mixtures in themselves, it has been thought necessary to replace them by different preparations.
Moreover, as regards faulty technique, the following excerpt from a Memorandum from DR. T. B. HILL Scott, M.O.H. for Antrim, is of special significance. Referring to the risks attached to the immunising process, he wrote in the Northern Whig Weekly, October 23rd, 1937:—
"In the hands of experts, careful both in regard to technique and the avoidance of immunising unsuitable subjects, such as those who might be in the process of developing diphtheria, the percentage of deaths would be very, very small, but imniunisation of the masses by busy, non-expert medical practitioners would probably greatly increase the percentage of disaster, and this factor must not be forgotten."
Even in the hands of experts, however, it was pointed out by C. C. OKELL, M.C., M.A., D.Sc., F.R.C.P., in the article quoted at the beginning of this chapter, mistakes "are made and are bound to be made sometime or other, even with the greatest vigilance. There are few immunologists responsible for the preparation of immunological reagents or doctors who have carried out immunisation on a large scale who have not had some hair-raising experiences." (The Lancet, Jan. 1st, 1938, p. 48.)
ALL THE DANGERS THAT NOW FOLLOW ARE INHERENT EFFECTS OF THE MIXTURES THEMSELVES, AND CANNOT BE ASCRIBED EITHER TO "TECHNICAL ACCIDENT" OR "HUMAN ERROR."
SECTION 7
THE INHERENT DANGERS OF "SCHICK" INOCULATION
THE INHERENT DANGERS OF "SCHICK" INOCULATION
Each immunising material has in turn been declared to be harmless, while each subsequent one has been recommended on the ground that its reactions may be expected to be less severe than those of its predecessor [As the Report of the Committee of the British Medical Association on Immunization including Vaccination (1935) stated:—The immunologist has evolved an almost bewildering multiplicity of prophylactics in his attempts to avoid reactions." (p. 12.)].
But, as a well-known bacteriologist, C. C. OKELL, M.C., M.A., Sc.D., F.R.C.P., stated in the Lancet, January 1st, 1938: "The risk of accidents must remain one of the snags in all forms of immunisation." (p. 48.)
In the circulars issued by public health authorities all over the country, it is continually stated that the injection of the mixture has been, and will be, attended by no ill effects.
The Chief Medical Officer of the Board of Education, SIR GEORGE NEWMAN, has described the procedure as a "safe, practical and efficient method of protection." (The Journal of Clinical Research, April, 1934, p. 64.)
No reference to the disasters which have been recorded in various parts of the world, nor to the severe reactions which are a frequent sequel to the inoculation, is made in these official statements, and even in the Memorandum (Med. 170), issued by the Ministry of Health for the guidance of Medical Officers of Health, only the barest mention of possible local reaction to toxoid is to be found.
In fact, the Medical Officer, January 9th, 1937, complained that : —
"There has been little advice from the Ministry of Health on the whole question of diphtheria prophylaxis. The only guidance from this source is the 170-Med., of November, 1932. In this, only one prophylactic, formol-toxoid, is mentioned. As the formol-toxoid technique requires a Maloney test which must be inspected in from 24-48 hours of performance, the method is quite inapplicable to clinics held once a week. Most general practitioners find the procedure too cumbersome and technical, so that, in point of fact, the majority of users of diphtheria prophylactics is left devoid of the slightest informatioii or help." (p. 12; my italics.)
With regard to the usual claim that the treatment is "painless and harmless," no more definite refutation could be imagined than that contained in the statement recently made by PROF. A. V. HILL, F.R.S., in the course of a defence of vivisection, that: —
"babies suffer when vaccinated, children when immunized against diphtheria, soldiers when inoculated against typhoid, etc." (The Leader, May 15th 1934, p. 2.)
Each of the chief immunising substances will now be discussed in turn : —IT IS TO BE PARTICULARLY NOTED THAT THE REACTIONS DESCRIBED ARE DIRECTLY DUE TO THE PECULIAR NATURE OF THE MATERIAL USED, AND ARE ADMITTEDLY NOT TO BE ATTRIBUTED TO ANY ERROR IN MANUFACTURE OR ADMINISTRATION.
This is a mixture of the toxin of diphtheria with antitoxic serum from a horse or goat.
1. The most serious danger is the occurrence of ANAPHYLAXIS and the ARTHUS PHENOMENON (Mass Gangrene).
Since this is shared by another preparation, TOXOID-ANTITOXIN, it is separately dealt with on pp. 82 to 91. An account will also be found in the Medical World, April 6th, 1934 (p. 151).
2. DR. C. D. MERCER, of West Union, Iowa, investigated the dangers of toxin-antitoxin and reported on them in the Annals of Internal Medicine (January, 1929, p. 668). He found that in 125 persons between the ages of six and twenty years immunised with three injections of T.A.T. supplied by the State Board of Health, the percentage of albuminuria was increased from the normal of 10 per cent, to 20 per cent. He concluded:—
"Toxin-antitoxin is not a harmless preparation and should not be given children in a haphazard way."
3. The British Medical Journal, March 23rd, 1929 (Epit. of curr. med. lit., p. 51), quotes a report from a Health Clinic in the city of Atlanta, U.S.A., which states that:—
"In the past three years the horse-serum product had given rise to severe reactions in at least 40 per cent. (of cases)."
4. An annotation in the Lancet, January 30th, 1932, contains a report of the investigations of two research workers (A. T. GLENNY and M. BARR):-
"It seems evident from these experiments that a toxin-antitoxin mixture which proved harmless when tested on guinea-pigs might be poisonous in a child, and it is not easy to devise any simple method of testing which would expose dangerous mixtures with certainty . . . It is clear that toxin-antitoxin mixtures should be given up." (p.252.)
As far back as 1922, SIR FREDERICK ANDREWES, addressing the Society of Medical Officers of Health (February 17th) warned them that:—
"The injection of toxin-antitoxin might be dangerous unless it were prepared by persons of the highest skill. Fatal cases had occurred abroad. There were only a few really competent for this work, and if the procedure were carried out on a large scale, a scheme of State control would be necessary."
5. Yet we find that, according to the Medical Officer, July 6th, 1929 (p. 2):—
"In New York the mixture is used more often than toxoid."
6. A. G. OGILVIE, M.B., M.R.C.P., Med. Registrar, Royal Victoria Infirmary. Newcastle-on-Tyne, confesses in the Medical World, December 5th, 1930:—
It is as well to mention here that reactions, sometimes severe, have occurred after T.A.T. injections . . ." (p. 351.)
7. In the Journal of the Medical Society of New Jersey, January, 1930, it is stated that : —
"The widespread use of toxin-antitoxin is too well known to necessitate elaboration. During the period covered by the increased use of toxin-antitoxin and therapeutic serums, the incidence of serum disease has also increased. . . . A 1927 report showed . . . that 28.2 per cent, of 1,199 patients who received diphtheria antitoxin subsequently developed serum disease."
8. In an article on "The Problem of Diphtheria " in the Lancet, January 26th, 1935, by J. S. ANDERSON, F. C. HAPPOLD, J. W. MCLEOD and J. G. THOMSON, it is stated:—
"Unfortunate accidents happened in the early days, but never in this country, as the result of the improper storage of the old toxin-antitoxin mixtures (T.A.T.). Toxin mixtures have not been used in England for several years. Formalinised toxin or toxoid is now invariably employed, alone or in combination with antitoxin; although a powerful prophylactic it is completely non-toxic." (p. 228.)
This last statement must, of course, be compared with the evidence regarding the reactions of these later mixtures, to be found in this section.
9. DR. J. MENTON, in a paper read before the North Staffordshire Medical Society and reported in the British Medical Journal, August 10th, 1935, declared-: —
"Toxin-antitoxin mixture is not now used in England, as it is rather risky, owing to the occurrence of dissociation of the toxin. Toxin-antitoxin fioccules are not in favour . . . The discarding of these toxin mixtures has eliminated those fatal and serious accidents which still arise on the Continent." (p. 248.)
This is formol toxoid to which a little antitoxin has been added to render it safer in the event of there being some reversion of toxoid to toxin
1. DR SAUNDERS M O H for Cork stated in an article on the subject of reactions in the Lancet April 15th, 1933 that:-
"It must not be forgotten that reactions of the utmost severity may occasionally be encountered with toxoid-antitoxin, and many cases come under our notice in which the whole of the upper arm has been involved in an intense inflammatory reaction accompanied by marked prostration (p 795)
2. DR GEO CHESNEY Assistant Medical Officer of Health for Poole, reported in the British Medical Journal July 15th 1933, a case of acute scarletiniform dermatitis following injection of toxoid antitoxin in a girl of 16. Two days after the second injection the skin rash "flared up in an acute dermatitis, spreading from the neck and chest to the back the abdomen then to the arms legs and head, until the whole body was involved with the exception of the hands and feet." This condition lasted between two and three weeks before showing signs of improvement (p 98)
3. The Lancet February 4th 1928 (p 249) reporting on ‘The Bundaberg Disaster ‘ (see p 63 par 6) stated:-
"Almost all the immunization in this country is carried out with toxoid-antitoxin mixture,"
4 In Recent Advances in Vaccine and Serum Therapy by ALEX FLEMING, F.R.C.S., and G. F. PETRIE, M.D. (Churchill, 1934), it is stated that —
"The most extensively used diphtheria prophylactic in England since 1924 has been a toxoid-antitoxin mixture." (p. 428.)
5. In answer to a question in the Rouse of Commons on March 15th 1934, "whether toxoid-antitoxin is still used for diphtheria immunisation in this country, and whether there has been any alteration in the strength of the mixtures used during the last twelve months"? the Minister of Health replied — The answer to the first part of the question is in the affirmative, and to the second in the negative [See also the Minister of Health’s answer to a further question by MR. TOM GROVES, on April 23rd, 1934, quoted on p. 88, post. The last part of this statement should be compared with that of DR. E. A. UNDERWOOD which follows in par. 6].
6. That there is dissatisfaction with toxoid-antitoxin is revealed by the statement of DR. E. ASHWORTH UNDERWOOD, Deputy M .O. H. for Leeds, namely, that on account of the "quite unsatisfactory results of the ordinary prophylactics such as T A M he had used formol toxoids of high values—between two and six times the strength of those employed in America (Medical Officer May 26th 1934)
7. In spite of this dissatisfaction however we find DR ELWIN H. T. NASH, Medical Officer for Heston and Isleworth, writing in the Medical World March 1st 1935: "I am working entirely with toxoid-antitoxin (T.A.M.) and do not intend to vary the process until . . . next March." (p. 11.)
8. In the comments of the Medical Officer of January 9th, 1937, on DR. BOUSFIELD’S article on immunisation, is a Table (p. 13) showing the percentage of undesirable reactions caused by various brands of immunising material. With Burroughs, Wellcome and Co.’s T.A.M. (Toxoid-Antitoxin Mixture) the percentage was 2.2; with Burroughs, Wellcome and Co.’s toxoid-antitoxin floccules it was 5.7; with Parke, Davis and Co.’s toxoid-antitoxin (goat) it was 8, and with Evans, Lescher and Webb’s toxoid-antitoxin floccules it was 4.6.
9. According to Evans’ Journal (New Series), Vol. 4, No. 2, November, 1938:—
"The disadvantages of T.A.M. are (a) that the serum in it may produce some susceptibility to horse protein and (b) the horse protein in it causes the formation of anti-bodies, and these hinder the anti-toxin response to the toxoid (c) it has the same tendency to produce reactions as F.T. Three injections are required." (p. 64.)
TOXOID-ANTITOXIN FLOCCULES (T.A.F.).
In order to avoid some of the unpleasant reactions associated with toxoid-antitoxin, especially in susceptible individuals, another mixture, T.A.F., was introduced. According to Evans’ Journal, Vol. 4, No. 2 (November, 1938, p. 64):—
"These are the floccules which form when toxoid and antitoxin are mixed in suitable proportions and consists of a combination of toxoid and antitoxin . . . It is suitable for the immunisation of adults, and is regarded as the safest of the prophylactics, [C.f. the percentage of reactions recorded in par. 8 above]…….but has the same disadvantage as T.A.M. resulting from the horse protein in its composition. Three injections are required."
In spite, however, of toxoid antitoxin floccules being considered the safest of all the prophylactics, it will be recalled that it was precisely this mixture which was held accountable for the particularly tragic disaster which occurred at Ring Irish College, Co. Waterford, in 1937. The case has already been mentioned on page 64; briefly, the disaster was one in which one little girl died and 23 others were made seriously ill through the injection of toxoid antitoxin floccules which had been supplied by a manufacturing firm of great repute. On enquiry, the Ministry of Health was satisfied that this firm had taken all possible precautions to prevent any mistake occurring in the production of the prophylactic. Since there was no doubt that the child died of generalised tuberculosis infection and that the other illnesses were considered to be of tuberculous nature, the statement made by the Ministry of Health that the bacteriological examination showed that the immunising mixture used was definitely free from tubercie bacilli, and that no substitution could have taken place, left the explanation of the tragedy a mystery [See Memorandum of Ministry of Health (June, 1937), quoted In the Vaccination Inquirer, August 2nd, 1987 (p. 135-6)]. Possibly some light on the problem may be shed by the following considerations.
That even with the milder form of mixture known as toxoid-antitoxin floccules there exists the danger of lighting up tubercular foci was pointed out in the Journal of the American Medical Association, May 23rd, 1936, in the course of a review of an article in which it had been recorded that children in a sanatorium for tuberculosis had shown distinct exacerbation of the disease after the third injection of either toxoid or toxoid-antitoxin floccules. Fuller details will be found under the next heading— "Formol-toxoid (paragraph 12); briefly, the author’s conclusion was: —
"In the form of the triple injection, toxoid as well as toxoid-antitoxin floccules is dangerous for children with active tuberculosis."
That the stronger toxoid may be dangerous in this respect had already been noted by AUBERTIN and BOUDOU in 1932 (see paragraph 8 on page 74).
TOXOID; FORMOL-TOXOID (F.T.); RAMON’S TOXOID; ANATOXINE
Toxoid is toxin which has been modified by combining it with formalin.
1.Parke, Davis and Co., in Therapeutic Notes, November, 1929, No, 5, state that:—
"Toxoid-antitoxin . . . is said to be free from the danger of the rather severe reactions which are occasionally produced by diphtheria toxoid alone." (See also Recent Advances in Vaccine and Serum Therapy. FLEMING and PETRIE, 1934, p. 429.)
2.In the Medical Officer, July 6th, 1929, it is stated :
"We know that undiluted diphtheria toxoid was used in London five years ago and the reactions in a small group of adults were so severe that its use was for a time abandoned."
"Park used toxoid in 1923 and has used it a good deal since. He has published some results showing a larger percentage of local and general reactions in patients receiving toxoid than in those receiving mixture (toxin-antitoxin)."
"Out of 144 patients in the series reported by G. F. and G. H. Dick who had been immunized with Ramon’s toxoid (anatoxine) 44 did not complete their treatment. The suggestion is that many of them failed to do so because of reactions, and the authors arc so impressed by this aspect of the matter that they give details of nine severe reactions in this group."
3. In an article in the Lancet, July 23rd, 1982, by R. A. O’BRIEN and H. J. PARISH, of the Wellcome Physiological Research Laboratories, it is stated that : —
"The only obstacle in the way of the universal use of toxoid is the tendency to cause local and general reactions in older children." (p. 176.)
4.According to the Lancet, March 17th, 1934:—
"The wider use of toxoid has been delayed here, just because of its tendency to produce more severe reactions than our public health authorities are accustomed to . . ." (p. 582.)
5.In Clinical Excerpts. Vol. 8, No. 11, November, 1933, it is stated: —
"The disadvantage of the toxoid is that it may produce unpleasant, though not dangerous, reactions in older children and adults."
6.In an editorial on "The Prevention of Diphtheria" in the Lancet, May 14th, 1932 (p. 1052), it is stated:—
"It has been objected, however, that toxoid at full strength, especially in adults, gives rise to troublesome reactions." (p. 1053.)
According to this article, SURGEON CAPT. DUDLEY, Medical Officer at Greenwich Hospital School, finds that not only are the reactions following Ramon’s toxoid more frequent age for age than after toxoid-antitoxin floccules, but that they are more severe. He considers "that in adults and protein-sensitive reactors, in whom toxoid may produce very unpleasant symptoms, floccules should always be used." (p. 1053.)
7.In the Memorandum (Med. 170) issued by the Ministry of Health in November, 1932, it is admitted that a strong reaction to formol toxoid may be expected IN 5 PER CENT. OF CHILDREN OF ALL AGES.
8. In Recent Advances in Vaccine and Serum Therapy (1934, p. 430), ALEX. FLEMING, F.R.C.S., and G. F. PETRIE, M.D., write : —
"It is recorded that in some children inoculations of toxoid have been followed by a flare up of tuberculous foci (Aubertin and Boudou, 1932)."
9.In The Journal of Clinical Research (Vol. XX, No. 2, April, 1934, p. 65), the statement is made:—
"It (toxoid antitoxin) does not cause the unpleasant reactions seen in the administration of toxoid." "Anatoxine . . .is apt to cause unpleasant reactions."
10. DR. E. ASHWORTH UNDERWOOD, Deputy M.O.H. for Leeds, writing of the immunisation of about 1,000 children with formol toxoid of high value, confessed : —
"A difficulty which is associated with the use of these powerful materials is that a certain proportion of children—roughly eight per cent.—are liable to show rather severe reactions after injection with the prophylactic." (Medical Officer, May 26th, 1934.)
11. Under the heading "Complications of Diphtheria Immunisation," the British Medical Journal, October 20th, 1934 (Epit. of curr. med. lit., p. 57), published the following report : —
"L.J. Ichard (These de Paris, 1934, No. 140), who records ten illustrative cases, seven of which occurred in children aged from 26 months to eight years, and three in adults, states that immunisation against diphtheria by anatoxin has given rise to the following series of complications: (1) local inflammatory reactions, such as oedema at the site of injection and nonsuppurative adenitis and a general febrile reaction; (2) less frequently, complications resembling serum sickness, such as urticaria and various eruptions with or without arthralgia or myalgia and even paresis of the lower limbs; (3) rarest of all, haemorrhagic complications, such as purpura haemorrhagica and haemorrhagic nephritis. The explanation of these complications is to be found in the individual who is specially sensitive to the proteins of the diphtheria bacillus and not in the anatoxin itself."
12.T he danger of causing a flare-up of tuberculous foci was again referred to in a review of an article in the Beitrage zur Clinik der Tuberculose (Berlin), which appeared in the Journal of the American Medical Association, May 23rd, 1936. The writer stated:—
"He found that, of 100 children who were given three injections of diphtheria toxoid, five showed exacerbations of the tuberculous process after the third injection. After that he used the milder acting toxoid-antitoxin floccules, but of thirty-five children who were immunised in this manner one showed a considerable exacerbation of the tuberculous process after the third injection.
"He concludes that, in the form of the triple injection, toxoid as well as toxoid-antitoxin floccules is dangerous for children with active tuberculosis." (p. 1861.)
13.Writing in the Lancet, September 11th, 1937, DR. H. A. RAEBURN stated that "it has long been realised that F.T. (formol toxoid) in sensitive individuals is capable of causing severe reactions." (p. 621.) He quoted the case of a girl of 14 years who was ill for three days as the result of a full dose of toxoid.
1. Introduced on account of the failure of toxoid-antitoxin (see pp. 54, 71), its "reactions" are described in an article by the Medical Officer of Health for Cork, DR. SAUNDERS, as varying from slight to severe, and as including abscess formation. (Lancet. April 15th, 1933.)
He wrote:—
"Generally speaking, the severe reactions to alum-toxoid have been more limited in extent" (than those of toxoid-antitoxin described on p. 71) "but have had sharply demarcated edges and have been of a more livid type." (p. 795.)
2. The Lancet, November 12th, 1932, contains an article dealing with alum toxoid, which has been used extensively by PARK and SHRODER in New York and by WELLS, GRAHAM and HAVENS in Alabama. It is there stated: —
"There seems to be a distinct tendency for the material to produce rather obstinate indurations, and occasionally even cold abscesses." (p. l069).
3. According to the Lancet, March 17th, 1934 (p. 582), PARK found that the reactions, though "not in the least harmful are annoying."
Referring to DR. SAUNDERS’ reports, it stated : —
"It was clear that the reactions he encountered were more numerous and more severe than would have followed the use of toxoid-antitoxin mixtures, toxoid-antitoxin floccules, and probably toxoid by itself."
"Baker and Gill found that local and general reactions were not any more severe with alum-toxoid than when ordinary toxoid was used. In this country such a statement might be taken as the faint praise that damns."
"In the Alabama series it is mentioned that some children showed local and even severe general reactions, and that eight developed abscesses which required incision . . ."
4. In Recent Advances in Vaccine and Serum Therapy (FLEMING and PETRIE, 1934), it is stated : —
"The addition of alum to toxoid increases its efficiency as an antigen, but it increases the reaction, and so it has attained no popularity for human immunization." (p. 430.)
5. GEORGE CHESNEY, M.B., D.P.H., Deputy Medical Officer of Health for Poole, wrote in the Medical Officer, May 16th, 1936, that in 1933 an alum formol-toxoid had been used to a limited extent in the clinic, but its extended use was not adopted" OWING TO MINOR LOCAL REACTION DIFFICULTIES." (p. 197.)
6. The British Medical Journal. September 14th, 1935, reported that D. G. LAI (Chinese Med. Journ., April, 1935, p. 340), inoculated 489 children, mostly of school age, with a single injection of alum toxoid. " The majority showed some local reaction, such as pain, swelling, induration and abscess, and 6 per cent. showed a general reaction, consisting of fever, headache and malaise."
DIPHTHERIA TOXOID, ALUM-PRECIPITATED (A.P.T.)
1. The very latest prophylactic to be issued is derived from diphtheria toxoid by precipitation with aluminium potassium sulphate. According to the makers (Mulford) it is not to be confused with alum toxoid. It has been used, they state, in Chicago since the autumn of 1932. After noting the "variability of commercial toxoid brands in general," they claim a further advantage of this preparation over others in that it is free from albumen, so that "severe reactions and the production of the anaphylactic state are avoided. In these days of serum treatment for a variety of diseases, with compulsory immunisation before journeys to other countries, this is of no small importance."
This is at least a confession of the dangerous nature of other prophylactics, and our suspicions of similar disadvantages in the newer preparations are by no means allayed when we read in the firm’s special Circular that:—
" Reactions are not greater than would be expected from ordinary Toxoid,"
"The resulting ‘lump’ may not disappear for four to five weekss." (Brochure issued by Sharpe and Dohme, Ltd., Mulford Biological Laboratories, May, 1934.)
2. But, as DR. GUY BOUSFIELD wrote in a letter to the British Medical Journal, January 26th, 1935, opposing the one-injection method : —
"People do not like their children to have lumps in the arms, such as are produced by alum-toxoids,"
He advocated, therefore, the use of the three injections of toxoid-antitoxin mixture, except for institutions where the children are all young and under medical supervision. Even then, he wrote, he would not use the" one-shot" alum-precipitated toxoid method personally; for, he stated : —
"All strong toxoid preparations are liable to produce quite a percentage of reactions in older children, and sometimes in younger ones, and even the most refined alum-precipitated varieties cannot be held to be above reproach in this respect." (p. 181.)
3. In the British Medical Journal, January 19th, 1935 (p. 103), C. J. McSwEENEY, M.D., M.R.C.P.I., D.P.H., described a series of experiments with various immunising mixtures in an article entitled "An Evaluation of Modern Diphtheria Prophylactics." It is of interest to note that he stated that the " experimental material" consisted of children drawn from two residential institutions, nine smaller homes, a hospital and two elementary schools, "-a total of 642 children," On page 105 he wrote : —
"In this experiment the alum-toxoid preparation used did not compare favourably with formol-toxoid or even with toxoid-antitoxin floccules, and its tendency to produce local redness is a contraindication to its general use outside institutions."
4. E, ASHWORTH UNDERWOOD, B.Sc,, M.B., D.P.H., writing on the use of alum-precipitated toxoid in the Lancet, January 19th, 1935, stated that :—
"A disadvantage in using it is the possibility of the occurrence of subcutaneous abscesses due to the retention of the alum in the tissues. In Saunders’ series of 579 cases, subcutaneous abscesses were met with four times." (p. 137.)
5. DR. W. B. R. MONTEITH, of Bourne, Lincs, in a letter to the The British Medical Journal, February 16th, 1935 (p. 332), reports the case of an adult of 40 who, seven days after inoculation with alum-precipitated toxoid, developed "an extremely painful aseptic abscess, the size of a bantam’s egg."
6. DR. J. MENTON, in a paper reported in the British Medical Journal, August 10th, 1935, declared that alum-precipitated toxoid, particularly recommended because one injection will sometimes immunise in a fortnight, "may cause severe local reactions in the form of induration or abscesses, and these are most apt to appear in children over two years of age, and in adults." (p. 249.)
7. WILLIAM PATTERSON, M.D., M.R.C.P., D.P.H., M.O.H. for Weybridge, comments in the British Medical Journal, November 16th, 1935, on DR. NAUGHTON’S suggestion that the local reactions shown by 20 out of 130 children injected with A.P.T. do not warrant apprehension, as follows : —
"I am afraid such a large proportion of local reactions would not be regarded without apprehension in Britain by parents of children living at borne, and would militate greatly against the success of future diphtheria immunization campaigns."
Relating his own experience with 20 Schick-positive children injected intramuscularly with A.P.T., he tells us that:—
"While the local reactions in these children, who were aged 6 to 15, were rather milder than those caused by Dr. Naughton’s subcutaneous injections, they were sufficiently severe to make me chary about using this preparation outside of residential institutions." (p. 971.)
8. In a letter published in the British Medical Journal, January 2nd, 1987, DR. GUY BOUSFIELD stated : —
"My view is that reactions are more common and more severe following the use of alum precipitated toxoid than is the case with any other prophylactic, except strong formol toxoid, whatever the past history of the subject as regards previous diphtheria or passive immunization." (p. 42.)
9. DR. J. C. SAUNDERS, M.D., N.U.I., D.P.H., Medical Officer of Health for Cork, a devoted supporter of immunisation, but disappointed with the failure of toxoid-antitoxin to prevent diphtheria, described in the Lancet, May 1st, 1937, his experiences with alum-precipitated toxoid. After mentioning that no less than 23.3 per cent. of children among his cases failed to present themselves for the full course of immunisation, "in spite of intensive following up," be went on to deal with types of "reactions" He wrote:—
"The reactions experienced with this lot of A.P.T. have been definitely less than with the older batches used some years ago, and this is especially so in regard to abscess formation." (p.1067.)
The total of all reactions recorded, however, was 14.5 per cent. Approximately 7 per cent. were mild, 5 per cent, moderate and 3 per cent. severe. In one case, a child of five "was brought by her mother three weeks after inoculation and then presented an abscess over the site of injection."
In his earlier cases DR. SAUNDERS had four abscesses out of 579 cases; in a Table giving the results of other authorities he showed that SHAFTON, in 1936, had 25 abscesses out of 101 cases treated with A.P.T.
With regard to the question of induration, be wrote: —
"It may be said that every case treated with A.P.T. develops induration in some form. Every case examined by us within five weeks presented it. Varying degrees of size and hardness were experienced." (p. 1068.)
10. In the Home Office Report on the Work of the Children’s Branch (1938) it is stated in regard to the " widespread extension of the practice" of immunisation against diphtheria in home Office Approved Schools: —
"The methods employed are not uniform . . . The prophylactic materials used are usually three injections of either toxoid anti-toxin floccules, or a toxoid anti-toxin mixture, or two injections of alum precipitated toxoid. Immunization by one dose of the latter is inadvisable, as it does not appear to give a reliable immunity, and has occasionally given rise to unpleasant reactions." (p. 83.)
For descriptive details of the various" immunising" preparations dealt with in this chapter, the reader should refer to Recent Advances in Vaccine and Serum Therapy, by ALEX. FLEMING, F.R.C.S., and G. F. PETRIE, M.D. (published by Churchill, 1934).
A TIMELY WARNING BY THE "MEDICAL WORLD."
The following comments upon all forms of immunising injections against diphtheria appeared in the official pages of the Medical World on September 9th, 1938 (page 101), and should be seriously taken to heart by all those who permit their enthusiasm for this type of preventive medicine to override saner judgment and foresight. The paragraph reads: —
"What happens if you inoculate a child against diphtheria, and then have to give some anti-tetanic serum, remembering always that the same child has already been vaccinated with calf lymph and may presently be called upon to sustain injection of T.A.B. vaccine before it stirs abroad? Are all these things of no more moment than so many changes in diet or is there some truth in the suggestion that injections of protein material are apt to leave behind specific sensitiveness or even the potentiality for non-specific reactions? As the practice of disease prevention advances in -the bands of those who have little real knowledge of the sick, the number of skin test inoculations and actual injections mounts up. It is just possible that the risk of getting some particular disease is really less than the risks which may attend the prevention of it. Some of these may be physical, but of these we know little because there has not been sufficient enquiry into the question. Of the psychological risks we are better informed. They ought not to be neglected. It is a common thing to find in the official reports of Medical Officers of Health some expression of regret that a proportion of parents proved disinclined to allow their children to be submitted to some test or injection. One may even encounter advocates of compulsory injections. That is a suggestion which certainly goes too far; what has happened to compulsory vaccination is evidence enough of that. But it is also true that parents are not necessarily wrong even if they seem to pit rather puny and elementary wits against- those of the trained Medical Officer of Health."
In the next chapter the question with which the foregoing paragraph opens is partly answered. Not only what may happen, but recorded instances of the disastrous results which actually have happened will be found described.
One very disquieting feature of many of the reports concerning reactions in young children is the not infrequent reference by the medical writer to the fact that, owing to the severity of these reactions, he would not advocate the use of the particular immunising material outside a residential institution [See p.78, par. 7 ante]. The implication is that, so long as there are no parents to object, the distressing symptoms caused the children by the injections may be disregarded by those acting as their " guardians" in the institutions in which they are being treated.
In one particular instance in which experiments were made to compare the effects of various immunising mixtures, the children inoculated for the purpose were actually described as "experimental material."[See p77,par.3,ante].
This is but one instance, related with unusual candour, of a type of experiment which indicates an attitude of mind that is the direct outcome of modern experimentation upon animals—an attitude of mind which subordinates every consideration to the desire to acquire knowledge and looks upon the subjects of the experimentation, be they animal or human, as merely means to an end—in other words, as " experimental material."
SECTION 8
DANGERS INHERENT IN ALL MIXTURES CONTAINING ANTITOXIN
THE ARTHUS PHENOMENON
ANAPHYLAXIS
MASS GANGRENE
DANGERS COMMON TO BOTH TOXIN-ANTITOXIN AND TOXOID-ANTITOXIN
The danger of producing ANAPHYLAXIS is common to all mixtures which contain ANTITOXIN, for this is derived from an animal serum [See Da. J. MENTON’S statement regarding the disadvantages of passive immunisation with antitoxin, p. 26, ante.].
It is important to note that in answer to a question in the House of Commons on March 15th, 1934, SIR HILTON YOUNG admitted that toxoid-antitoxin was still used in this country, and that there had been no alteration in the strength of the mixture during the preceding twelve months. (See p. 71, par. 5.)
1. In Therapeutic Notes (November, 1929, No. 5), issued by Parke, Davis and Co., it is stated: —"It is obvious that a preparation containing horse-serum introduces the possibility of sensitizing the recipient to a subsequent dose of horse-serum, as the great majority of antitoxins employed therapeutically are developed in this animal."
2. Writing in the Journal of the Americais Medical Association, January 9th, 1926, DR. CHESTER STEWART, Assistant Professor of Pediatrics in the University of Minnesota Medical School, warns his readers that: —As a result of the widespread employment of toxin-antitoxin preparations for active immunization of children against diphtheria, clinicians undoubtedly will encounter an increased frequency of the incidence of anaphylactic reaction following subsequent administration of serums to these sensitized patients." (p. 113.)
One of his cases, who had been immunised a year previously, was injected with antitetanic serum and at once developed alarming reactions: very rapid breathing and diffuse redness of the skin which, a week later, broke out into enormous weals all over the body, with severe swelling of the tongue, face, hands and feet; this was followed at intervals of a few days by four similar attacks.
In six other cases the symptoms, writes the author, "were of such severity as to be alarming "; in one case the temperature rose to 104° F., and the child had severe vomiting attacks every half-hour for twelve hours.
Justification for DR. CHESTER STEWART’S prophecy as to the future is provided by: —
(a) The statement of H. A. RAEBURN, M.D., M.R.C.P., D.P.H., in the Lancet, September 11th, 1937 (p. 623), that GORDON and CRESSWELL had recorded reactions in 74.1 per cent, of scarlet fever cases who had, previous to injection with serum, been immunised against diphtheria and in only 18 per cent, of non immunised patients.
(b) The statement in Therapeutic Notes, December, 1938, that: —
"The increasing use of serums and antitoxins in the treatment and prophylaxis of disease has resulted in a larger proportion of people becoming sensitized to horse-serum products; this gives rise to an increasing incidence of serum reactions.
"Of one thousand persons treated with tetanus antitoxin, 15.2 per cent, developed generalized serum reactions. . . Approximately 25 per cent. of the reactions were severe and a comparatively small number were alarming.
"Possibly the chief factor influencing the higher percentage of reactions in young persons is the fact that a larger number of young people have previously received injections of horse-serum products, as, for instance, in some forms of diphtheria prophylactic made with horse-serum." (p. 184; my italics.)
(c) The fact th.at results even more serious in their nature than the foregoing have been recorded in recent years. The following example is taken from a letter which appeared in the Lancet, October 20th, 1934, and in which DR. SINCLAIR MILLER, of Harrogate, expressed the opinion that "the risk of serum anaphylaxis is probably greater than hitherto we have imagined." He went on to describe the case of a boy of 14 who gave no history of asthma and had had no serum previously except the smalr amount contained in the three prophylactic doses of T.A.F. given two years before. Within a minute or two of receiving an intramuscular injection of 5 c.c. of anti-scarlet fever serum sickness and vomiting occurred; the boy rapidly became collapsed and pulseless, with lips, tongue and face markedly swollen. Despite injections of adrenalin and artificial respiration " the cedema of mouth and air-passages was so great that little progress was made. There were never any signs of recovery." (p. 897.)
The occurrence of cases such as this one is a striking commentary on the assertion of GEORGE CHESNEY, M.B., D.P.H., regarding the risk of sensitisation by toxoid-antitoxin.. Writing in the Medical Officer, July 7th, 1934, he stated : —
"The suggestion that the presence of horse serum in this prophylactic would cause sensitization and give rise to possible risk in the event of a curative injection of horse serum being required at a later date has not so far been substantiated in practice." (p. 5.)
On the contrary, it is quite clear that the suggestion has been fully substantiated in practice.
Stedman’s Medical Dictionary, 1923, defines it as: —
"A phenomenon of anaphylaxis in which a rabbit, after receiving several injections of normal horse serum, develops an abscess, edema, or gangrene at the site of the last injection, becomes cachectic, and dies." (See also pp. 90, 91, post.)
It was first described by MAURICE ARTHUS, a French bacteriologist in 1903. LUCAS and GAY called attention to similar effects in children in 1909. DR; HARRISON TUMPEER, in an article in the American Journal of Diseases of Children, February, 1933 (pp.343-354), declared that; —
"Undoubtedly subsequent reactions in the nature of the Arthus phenomenon occurred following additional use of horse serum for other reasons, but were disregarded or not sufficiently appreciated until 1927."
He went on to add : —
"With the advent of the antitoxin era, a new situation developed in which sensitisation to horse serum was produced by three injections at weekly intervals of the minute quantities of horse serum present in the ordinary toxin-antitoxin mixtures...."
1. In 1927 GATEWOOD and BALDRIDGE described six cases, the severest of which occurred in a nurse of twenty-five. The particulars they gave in the Journal of the American Medical Association, April 2nd, 1927 (p. 1068) are briefly as follows: —
The nurse was Schick-negative in January, 1925, but, "in spite of this she was given toxin-antitoxin mixture in three doses, February 6th, 13th and 20th." She developed diphtheria in November, 1925, and was given antitoxic serum in one arm and the corresponding hip. This was followed by acute general enlargement of the superficial lymph nodes. On the ninth day a further injection of serum in the other arm and corresponding thigh resulted in the arm becoming red, swollen and tender, and by the second day both arm and leg were twice the normal sire. By the ninth day after the second injection the skin of the thigh lesion had become a black eschar; free incision yielded no pus although the tissue was necrotic. On the twenty-sixth day the discharge from the wound became purulent, On incision, "the abscess cavity was found to extend from the knee to the hip and around the thigh to the inner aspect. In the previous wound there presented a mass of necrotic tissue which was removed. It involved subcutaneous fat, fascia lata and muscle, and was a mass the size of a fist," The left arm, which had undergone all the changes of the thigh, was later incised, yielding thick yellow necrotic material. The nurse eventually recovered.
The authors predicted that the Arthus phenomenon might logically be expected to be reported more frequently with the increased use of horse-serum.
Fig 1 & Fig 2:
2. In 1931, DR, I. HARRISON TUMPEER described the following case (Journal of American Medical Association, April 25th, 1931, pp, 137a-6):-
A girl of five years had received the usual three injections of toxin-antitoxin in 1926 when one year old. In 1927 she was pronounced Schick-negative. She developed diphtheria in 1930, and an injection of serum was given in the left gluteal region, followed three days later by a second dose on the opposite side. In three bours the buttock began to swell and became extremely tender, until eventually the whole region became black and gangrenous. By the ninth day a deep area of ulceration appeared at the margin separating the necrotic tissue from the normal. (See Fig. 1.)
On the twelfth day the child began to complain of extreme pain over the right lower quadrant of this area, and an incision yielded thick yellow pus. From now onwards the condition spread over the abdominal wall and thigh until the sixteenth day, when a large necrotic mass 6" by 8" was cut away under anaesthesia. The author writes; "This large piece of gangrenous skin with subcutaneous fat and fascia was lifted off much as a lid from a stove... . . the underlying muscles lay exposed almost entirely independent of fascia which aloughed, and a large amount of which had come away in the discharge. After apposition, the muscles lay exposed much as in an anatomic dissection." (Figs. 2, 3.) In spite of assiduous irrigation of the wound she became rapidly worse, suffering considerable pain. Following a blood transfusion on the twenty-seventh day of illness, she became cyanotic, vomited, lost consciousness and died a few hours afterwards.
Fig 3 & Fig 4
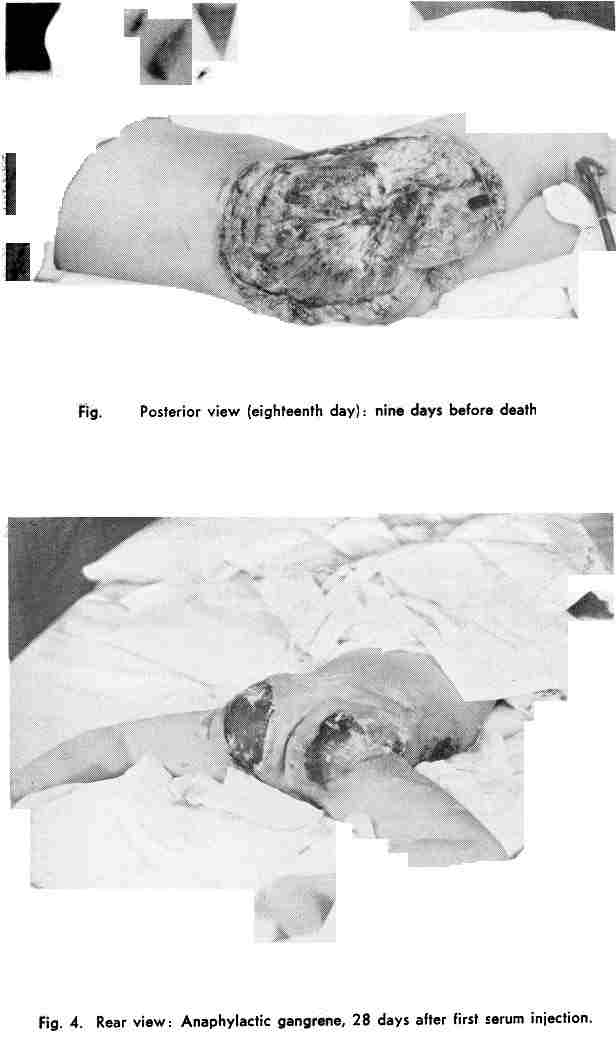
Fig 5 & Fig 6
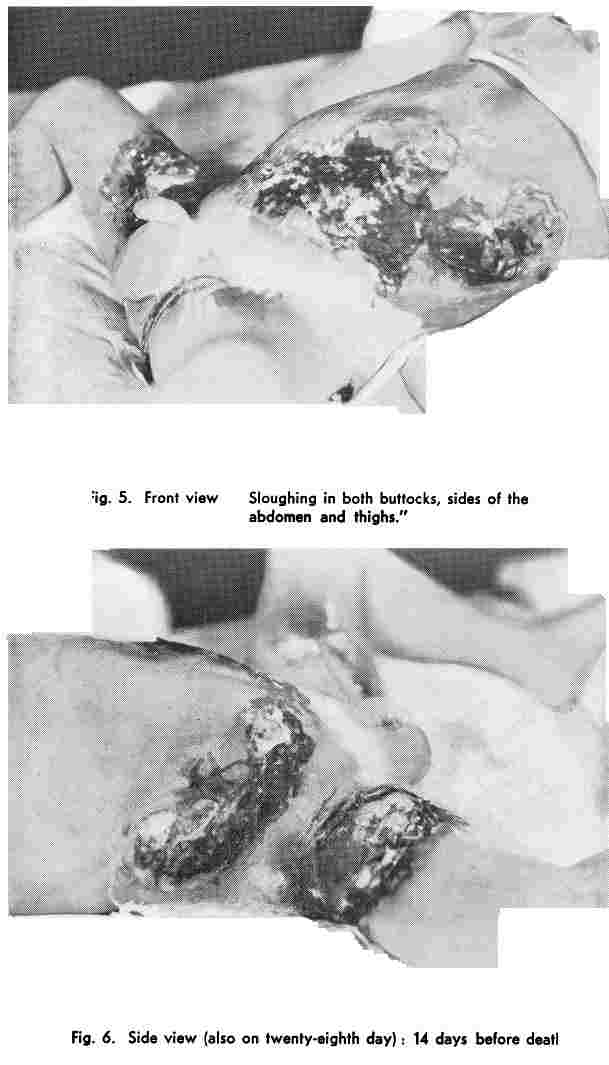 3. The third case was reported by
DR. H. E. IRISH and DR. E. C. REYNOLDS in 1933, and occurred in a boy aged two years and
four months. (Journal of American Medical Association, February 18th, 1938, p.
490.) He developed symptoms suggesting meningitis and was given three injections of
anti-meningococcie serum on three successive days, and a further dose four days later. The
three usual toxin-antitoxin inoculations had been performed at the age of eleven months.
The serum was injected into the buttocks and was followed by an urticarial eruption over
the entire body, the edematous swelling of the face being sufficient to close the eyes.
Delirium with a temperature of 103° F. persisted for three days, when he became rigid. He
was then given a further injection of serum in the left buttock; within an hour the site
became purple, and on the following day a similar injection into the right buttock
resulted in a similar reaction. During the next few days the areas of purple swelling
extended from the buttocks over the front of the abdomen and right thigh, and large blebs
about one and a half inches in diameter appeared; six days later these gave rise to a
bloody watery discharge.
3. The third case was reported by
DR. H. E. IRISH and DR. E. C. REYNOLDS in 1933, and occurred in a boy aged two years and
four months. (Journal of American Medical Association, February 18th, 1938, p.
490.) He developed symptoms suggesting meningitis and was given three injections of
anti-meningococcie serum on three successive days, and a further dose four days later. The
three usual toxin-antitoxin inoculations had been performed at the age of eleven months.
The serum was injected into the buttocks and was followed by an urticarial eruption over
the entire body, the edematous swelling of the face being sufficient to close the eyes.
Delirium with a temperature of 103° F. persisted for three days, when he became rigid. He
was then given a further injection of serum in the left buttock; within an hour the site
became purple, and on the following day a similar injection into the right buttock
resulted in a similar reaction. During the next few days the areas of purple swelling
extended from the buttocks over the front of the abdomen and right thigh, and large blebs
about one and a half inches in diameter appeared; six days later these gave rise to a
bloody watery discharge.
At this time the child was admitted into hospital, and presented gangrenous areas on both buttocks, both sides of the abdomen, and the thighs. There was a patch of pneumonia in the right lung and a left otitis media. Despite the removal of large masses of necrotic tissues, surgical drainage and three blood transfusions, the child died in twenty-one days from admission to hospital. (See Figs. 4, 5 and 6.)
It is necessary to emphasise once more that this phenomenon of mass gangrene is one which may occur without previous warning in any child who has been at any time subjected to any so-called immunisiug inoculations containing antitoxin, should a further injection of horse-serum be given. It is not a particularly comforting thought for any parent to feel that the possibility of such a tragedy hangs over his child for an indefinite period, no matter how carefully the injection has been carried out, and despite all precautions in manufacture. The danger is inherent in serum therapy [See paragraph at the end of this Section, dealing with the denial of this statement on the part of DR. G. H. DART, Medical Officer of Health for Hackney, London]
DR. HARRISON TUMPEER remarks:
"It is reasonable to suppose that many individuals inoculated with toxin-antitoxin derived from horse-serum might subsequently require horse-serum for such conditions as scarlet fever, pneumonia, tetanus, hemorrhage, or even diphtheria itself. In such individuals there would be present to some degree at least. the laboratory conditions of Arthus." (Jour, of Amer. Med. Assoc., April 25th, 1931, p. 1373.)
LONGCOPE and RAKEMANN have stated that "the injection of horse-serum in small or large amounts in human beings is always followed sooner or later by ‘the development of (specific) hypersensitiveness of the skin . . ." (Jour. of Exper. Med., 27.341; 1918.)
Nor is the problem affected by the smallness of the dose;[ROSENAU and ANDERSON (1906, 1907) noted that the amount of serum required to produce sensitization in guinea-pigs was extremely small, as little as one millionth of a cubic centimetre induced typical hypersensitiveness. (PROF. W. W. C. TOPLEY, in An Outline of lmmnunity, 1933, p. 77.)] for in an article on this very point in The Journal of Immunology (Vol. IX, No. 1, January, 1924, p. 7), DR. S. B. H0OEER, of Boston, writes: —
"That such a tiny amount of horse-serum (about 0.01 mil. in the total individual dose of toxin-antitoxin, and 0.005 mil, in the test dose) should suffice to develop allergic conditions in previously non-sensitive human beings was regarded as a phenomenon of considerable biological interest."
GATEWOOD and BALDRIDGE (Jour. of Amer. Med. Assoc., April 2nd, 1937, p. 1071), after referring to the definite demonstration by Hooker of the production of skin hypersensitiveness in otherwise normal and insensitive individuals by the injection of toxin-antitoxin, go on to declare that: —
"The statement from most commercial biological laboratories as well as many workers in the field of immunity, that the amount of horse-serum in toxin-antitoxin mixture is too small to be sensitising, seems to us to be untenable."
This conclusion is borne out by a recent fatal case (see p. 83, ante), and by DR. HARRISON TUMPEER’S experience that:—
"Minute quantities of foreign protein are highly antigenic. Clinically this fact has become amply demonstrated in some of the severe reactions to scarlet fever antitoxin which resulted in the accusation of extreme toxicity against that agent. The accusers had overlooked the fact that most of the children receiving scarlet fever antitoxin had previously received horse-serum in the form of toxin-antitoxin." (Jour. of Amer. Med.Assoc., April 25th, 1931, p. 1375.)
The probable frequency of such occurrences to be expected in actual practice is indicated by GATEWOOD and BALDRIDGE in a Table which they give showing the percentage of reactions after giving diphtheria antitoxin in a series of cases. (Jour. of Amer. Med. Assoc., April 2nd, 1927,
| No of cases | Immediate local reactions | Delayed local reaction | General reaction | Total reactions | |
| Toxin-antitoxin. No other serum | 87 | 27 | 17 | 1 | 50.5% |
| TAT. Also therapeutic dose of serum. No toxin-antitoxin | 26 | 20 | 2 | 0 | 84.6% |
| Neither TAT nor other serum given previously | 19 | 9 | 3 | 0 | 63.1% |
| 158 | 19 | 1 | 0 | 12.6% |
In the Journal of Immunology (Vol. IX, No. 1, January, 1924, p. 17), further Tables are given showing that over 70 per cent. of children (116) who had been immunised by toxin-antitoxin (three injections) were hypersensitive to horse-serum, compared with 50 per cent. of those children who had no previous injections (90). In adults the percentage of hypersensitiveness was 90 in the immunised, compared with 74 in those who had not received any injection of serum or toxin-antitoxin [See also references to investigations by HooKER, PARK, LONGCOPE, RACKMAN, GORDON, CRESSWELL and MACKENZIE in An Outline of Immunity (1933). by PROF. W. W. C. T0PLEY (p. 209)].
The whole difficulty is increased by the fact that there is no certain method of deciding beforehand if any given case is likely to react unfavourably; for, as DR. HARRISON TUMPEER states:
"Reactions may occur even when skin tests are negative." (Jour. Of Amer. Med. Ass, April 2, 1927 p1376)
Although the foregoing reactions were in connection with TOXIN-ANTITOXIN, the danger of their occurrence is equally great in the Case of TOXOID-ANTITOXIN a prepatation declared by the Minister of Health to be in use in this country [See Hansard, March 15, 1934, quoted on page 71, par5], since the substance which causes them, the ANTITOXIN, IS PRESENT IN BOTH.
DR J. CHAMBERLAIN, in his prize essay read to the Guy’s Hospital Physical Society, on " The Nature and Clinical Significance of Anaphylaxis," in 1931, declared:—
"The increasing frequency with which human interference permits injections of antigenic substances into the circulating blood, betokens an increasing number of fatal anaphylactic reactions and other less significant forms of sensitization." (Medical World, Jan. 2nd, 1931, P. 476.)
A copy of the Medical World, April 6th, 1934, containing an account of the dangers of Anaphylaxis,[Some Little Understood Effects of Serum Therapy, by M. BEDDOW BAYLY, M.R.C.S., L.R.C.P.] with illustrations of the cases of mass gangrene already described, having been sent to each Member of Parliament, the Minister of Health was asked by MR. GROVES on April 23rd, 1934 :—
Whether his attention had been called to cases that have occurred of anaphylaxis due to the injection of toxin-antitoxin; and whether, in view of the use in this country of toxoid antitoxin for diphtheria immunization he will take steps to safeguard the public against possible similar results of such injections?
The Minister of Health, SIR HILTON YOUNG, replied —
The answer to the first part of the question is in the affirmative. With regard to the second part, anaphylaxis is not a phenomenon peculiar to diphtheria immunization. I am advised that the relevant facts are widely recognised, and I do not consider it necessary to take any special action in the matter."
Since then two further cases of anaphylactic mass gangrene have come to our notice. One, the less severe, since the patient recovered, was that of a nurse who had been "immunised" and found Schick-negative; three years later she developed diphtheria, was admitted to hospital, and given an injection of antitoxic serum. The severe reactions so closely resembled those described in the case (1) on page 84 that the details may be omitted: they are fully reported by JOHN A. MARONEY, M.D., in The New England Journal of Medicine, July 19th, 1934 (p. 106).
The second case, which ended fatally, is fully described in a Report by FREDERICK E. Ross, M.D., in the Journal of the American Medical Association, Vol. 103, No. 8 (August 26th, 1934, p. 563). He writes:—
"A boy, aged 4 years, had been given toxin-antitoxin for diphtheria immunization a year previously. November 22nd (1933?), he sustained a scalp injury and the attending physician administered a prophylactic injection of tetanus antitoxin. Three days later he had a temperature of 104°F., a generalized erythematous rash, vomiting and a sore throat with cervical adenitis. The symptoms so closely resembled those of scarlet fever that the physician administered a therapeutic injection of scarlet fever streptococcus antitoxin in the buttock. The efflorescence cleared up in a few hours, but the site of the injection immediately became indurated and erythematous, and a lesion developed which spread with such fulminating intensity that when seen, December 1st, the skin and subcutaneous tissues of the entire thigh, hip and abdomen were involved in a large necrotic sloughing mass. The patient died as the result of sepsis that evening."
ACUTE ANAPHYLACTIC SHOCK FOLLOWING INTRACUTANEOUS TEST FOR SENSITIVITY TO HORSE-SERUM.
In order to avoid the possibility of such " accidents" following the administration of serum, some workers have suggested that a preliminaiy skin-test for sensitivity to horse-serum should be carried out [See pamphlet. "The Dosage of Antitoxin in Diphtheria," issued November, 1936, by the London County Council, pages 13-14].
Not only, however, is the test useless because, as DR. HARRISON TRUMPEER [Jour. of Amer. Med. Assoc., April 2nd, 1927, p. 1376], has pointed out, "reactions may occur even when the skin tests are negative,’ [In the pamphlet, "The Dosage of Antitoxin in Diphtheria," issued November, 1996, by the London County Council, It is stated on page 13: ‘severe reactions have been reported in people with a negative skin test."] but the test itself is not devoid of risk.
This was indicated in a communication to the New England Journal of Medicine, January 3rd, 1935 (p. 10), from HAROLD J. FREEDMAN, M.D., who reported a fatal case of anaphylactic shock following such a test in a boy of six. Twenty days before coming to the clinic this boy had received a dose of toxin-antitoxin, which was followed by asthma and urticaria. To test this he was given an intracutaneous injection of 0.05 c,c, of horse-serum.
Two minutes after the injection a large wheal appeared and urticaria spread over face and body. An injection of adrenalin (0.3 c.c.) was given, and one minute later "the child doubled up and complained of abdominal pain." In a few seconds be became intensely cyanosed and respirations ceased. All means of restoration, including further injections of adrenalin and artificial respiration, were of no avail, and "the child died about eight minutes after the test dose."
DR. FREEDMAN also mentioned a number of other instances in which a minute dose of foreign protein injected intracutaneously as a test had been followed by death, thus emphasising the risk which attend all such procedures. Allergic reactions following the Schick test have already been described in an earlier chapter (p. 35.)
A MEDICAL OFFICER OF HEALTH’S CHALLENGE.
Following the publication in the Medical World, April 6th, 1934, of an article entitled "Some Little Understood Effects of Serum Therapy," and containing a description of the cases of mass gangrene which have been dealt with in the first part of this Section, together with the illustrations which accompany them, G. H. DART, M.D., M.R.C.P., D.P.H., LL.B., Medical Officer of Health for Hackney, issued, in November, 1934, an official Memorandum to the Public Health Committee of Hackney Borough Council in which he sought to show that such effects could not have been caused by the injected material.
These results," he wrote, " are not inherent in the properties of animal serum and these cases of ‘massive gangrene’ are accidents that should never occur anywhere. I have consulted some of the leading authorities and satisfied myself on this point."
One can only say that Dr. Dart has quite clearly been seriously misinformed, for there does not appear to be any divergence of opinion on the part of responsible bacteriologists. Anaphylactic gangrene is universally recognised as a phenomenon due entirely to the injection of foreign protein such as that contained in animal serum; if there are any authorities of standing who deny this, they have not been brought to my knowledge. At any rate, the authorities already quoted.—TUMPEER, LONGCOPE, RACKEMANN, HOOKER, GATEWOOD, BALDREIDGE and CHAMBERLAIN----present an array of opinion which it is impossible lightly to disregard.
Most medical men will be familiar with the Medical Research Council’s monumental work, A System of Bacteriology in Relation to Medicine (1931). On page 457 of Vol. VI will be found the following : —
"Anaphylaxis is best defined in terms of the experimental facts. These are: (1) Active sensitization, i.e., that the parenteral (injection) administration of any one class of substance, the anaphylactogens (which are generally non-toxic and include, especially, the soluble proteins), makes animals sensitive . . . so that injection of the same substance into their circulating blood, the assaulting dose, sets up a characteristic train of symptoms, the anaphylactic shock; injection into the subcutaneous tissue sets up a local inflammatory reaction which varies from slight oedema to complete necrosis, and is known as the phenomenon of Arthus or local anaphylaxis."
"This, the phenomenon of Arthus, is not confined to the rabbit, but can be induced in all animals including man, though as a rule, the reaction is mild and stops short of necrosis." (Ibid. p 462; writer’s italics.)
Furthermore, in Parke, Davis and Co.’s publication, Therapeutic Notes, March, 1937 (p. 26), it is stated of Local Tissue Anaphylaxis : —
"This is a local reaction (reported in a few instances under the name ‘Arthus Phenomenon’) developing in the subcutaneous and muscular tissues when antitoxin is re-injected after a certain number of days. If re-injections are made within five days, this phenomenon is usually not observed. The symptoms, which are slow in developing, may result in considerable sloughing of tissue."
DR. DART’S claim that in this country such accidents could not occur unless the "Therapeutic Substances Act and Regulations were permitted to fall into abeyance," is therefore pointless; there is no evidence that the preparations used for injection were contaminated. It is true that Dr. Dart adds another proviso: "unless there was the very gravest negligence or accident "; but we need not envisage such an unlikely happening in this country, and it is scarcely courteous to suggest, as Dr. Dart does, that these deaths from mass gangrene were due to malpractice on the part of our American colleagues.
DR. DART stigmatised my criticisms of medical treatment as "an entirely unjustifiable slur on the integrity of the medical profession," but the fact is that the boot is on the other foot. Nowhere, I submit, have I expressed anything so derogatory to the medical profession as DR. DART’S own suggestion regarding the real cause of these " accidents." Referring to the third case (described on page 85) he wrote: —
"In this case, so mismanaged, it might throw further light on the subject to enquire where and how the serum was given. It would not be surprising under the circumstances to find that the serum had been given to the child IN THE SCULLERY FROM A BICYCLE PUMP WITH A DIRTY NEEDLE." (My emphasis.)
It is, of course, quite easy to make such imputations against doctors in America, but, I think, the reader will agree it is hardly a reasonable substitute for scientific argument.
SECTION 9: STATISTICAL FALLACIES
To gain some idea of the confusion that obtains in the compilation of hospital statistics, it is only necessary to glance at the following Table, which is derived from the Annual Reports of the Birmingham City Infectious Diseases Hospitals, and shows the number of cases sent in by medical practitioners as DIPHTHERIA and the percentage "requiring revision of diagnosis ": —
Year. Number sent in as diphtheria Number requiring revision of diagnosis
1928 1,909
458 (23.9 per cent.)
1929 2,099
703 (33.5 per cent.)
1930 2,162
744 (34.5 per cent.)
1931 1,728
690 (39.9 per cent.)
1932 1,156
609 (52.7percent.)
1933 788
441 (55.8 per cent.)
1934 1,551
585 (50.9 per cent.)
1935 1,796
628 (34.9 per cent.)
1936 1,620
510 (31.4 percent.)
1937 2,049
743 (36.2 per cent.)
In 1932, 303 out of the 609 revisions were finally diagnosed as TONSILLITIS. In 1933, 285 out of 441 revisions were also finally classified as TONSILLITIS. The Annual Report for 1933 states: —
"This very large number of cases of tonsillitis is undoubtedly due to the fact that, as in former years, virulence tests were carried out as an aid in the bacteriological diagnosis of doubtful cases—in addition to the use of the Schick test. Many of these cases would undoubtedly have been called mild cases of diphtheria if the microscope were the only means of diagnosis."
In 1934, 368 revisions; in 1935, 306; in 1936, 222; and in 1937, 321, were finally diagnosed as tonsillitis.
In reply to a question in the House of Commons (March 19th, 1935), the Minister of Health said that between 1931 and 1933 there had been 30 cases among those re-diagnosed as tonsillitis in Birmingham in which the patient had been immunised previously.
In the 1932 Annual Report of the City of Birmingham Infectious Diseases Hospitals is a table of 26 immunised cases which had been sent in by doctors as DIPHTHERIA, but in which the " final diagnosis was based on (1) the clinical evidence; (2) the Schick test; and (3) the result of the bacteriological investigation (virulence test on guinea pigs). All those found to be Schicknegative were classified to diseases other than diphtheria, in spite of the fact that, as we have seen (see page 30 ante), many authorities have reported undoubted cases of diphtheria in patients giving a Schick-negative reaction.
A NEW NAME FOR DIPTHERIA IN THE IMMUNISED
It is obvious that this practice of screening statistics, apparently in order to suppress facts unfavourable to immunisation, invalidates most of the evidence brought forward by the supporters of immunisation. They have even gone so far as to invent a new disease known as TONSILLITIS IN SCHICK-NEGATIVE CARRIERS to describe cases of apparent diphtheria in persons "who had at one time or another been Schick-negative." This is mentioned by H. J. PARISH, M.D., M.R.C.P., D.P.H., of the Wellcome Research Laboratories in an article in the Lancet, March 16th, 1935. (p. 600.)
It will be noted that whereas at the time of the introduction of antitoxin in 1894 the final diagnosis of diphtheria was changed from clinical to bacteriological and resulted in the inclusion of thousands of ordinary sore throats in the diphtheria statistics and a consequent fall in the case mortality [See pp. 6 and 13, par. 2] (a manoeuvre favourable to the use of the antitoxin), the present change, in abandoning the hitherto accepted bacteriological diagnosis, automatically reduces the number of cases of diphtheria and therefore produces figures apparently favourable to immunisation, the latest craze.
MILD CASES IN "IMMUNISED" cannot BE DIPHTHERIA.
But in addition to this fundamental change of front there has to be mentioned another alteration in diagnosis. This consists in the refusal to classify cases as diphtheria among the immunised, on the ground that they only present mild symptoms. According to the Medical Officer of Health for Ipswich (see East Anglian Times, February 22nd, 1934), it has become the practice not to regard as diphtheria persons who, after immunisation, develop sore throats even though the presence of the Klebs-Loeffler bacilli (hitherto considered to be diagnostic of the disease) can be demonstrated in them.
Such a manoeuvre is not only bound to falsify all subsequent vital statistics, but can be shown to be unjustifiable on grounds of medical pathology, for the assumption that mild cases are not likely to be diphtheria is not borne out by historical records.
(a) Clinical Excerpts of January, 1934, contains an account of the disease as it occurred in the middle of the 18th century, taken from JOHN FOTHERGILL’S Account of the Sore Throat Attended with Ulcers. From this it appears that " in Kidderminster, of 242 cases treated with ‘bark and opium,’ only seven died, and of these six had neglected early treatment " (a case-fatality of only 2.8 per cent.).
(b) In a paper read before a branch of the British Medical Association, and reported in the Brit. Med. Jour., December 7th, 1861, DR. WILLIAM CARR said : —
"From my personal observations of this disease there are two forms of diphtheria: (1) the malignant and acute; (2) the simple. The former has a high rate of mortality, higher than that of any other disease with which I am acquainted; the latter, on the contrary, seldom proves fatal." (p. 606.)
(c) In a series of 6,800 cases of diphtheria treated without serum in the hospitals of the Metropolitan Asylums Board between 1900 and 1909 the case fatality-rate was only 3.02 per cent.
Moreover, this exclusion of mild cases among the " immunised" from the classification of diphtheria is seen to be doubly disingenuous when it is recalled that one of the claims made in favour of immunisation is that when diphtheria does occur in such persons it is invariably mild, or modified [DR. Guy BOUSFIELD- in a letter to the Vaccination Inquirer, January 11th, 1936, stated that "such attacks are modified, usually of a trivial nature, and, more important still, that grave sequelae or death from the disease are practically unknown." (Cf. page 55.)].
TYPICAL CLINICAL CASES NOT DIPHTHERIA IN "IMMUNISED" UNLESS KLEBS-LOEFFLER BACILLUS PRESENT.
A further complication in diagnosis has been introduced by the Medical Research Council, who state in their Special Report, No. 115 (1927), that before any diagnosis of diphtheria can be made in a Schick-negative reactor, even though he presents all the clinical features of the disease,
"Diphtheria bacilli must be obtained in culture from the individual’s throat or nose, and proved virulent by guinea-pig test." (p. 17.)
As we have seen previously, the K.L.B. (diphtheria germ) may be absent in as many as 40 per cent. of cases of clinical diphtheria (see p. 6); so that using one or other of these methods of "exclusion ‘ it would be quite possible to rule out a very large proportion of cases occurring in Schick "immunised" or negative persons from the classification of diphtheria.
The second source of error lies in the omission to present comparable classes of children when comparing the incidence among inoculated with that among uninoculated.
When the differences in the social status, hygienic surroundings, nutrition and general state of health are considered, the possibilities of error due to these factors being ignored are seen to be enormous.
Age classification is another factor which it can he demonstrated has led to serious errors.
DR. J. F. C. HASLAM points out : —
"The incidence and mortality rates of diphtheria vary from age to age."
And referring to American statistics he says:
"There is nothing in the data cited in support of this or of most other immunisation campaigns to show that the groups compared were of similar susceptibility or were exposed to equal risk." (" Recent Advances in Preventive Medicine " [Churchill, 1930], p. 296.)
In DR. GRAHAM FORBES’ Report (No. 115) issued by the Medical Research Council (1927) it will be found that 76 per cent. of the children immunised (in Edinburgh) were between 5 and 10 years of age, only 21.2 per cent. being under this age. (p. 61.)
But of the total number of deaths from diphtheria by far the larger portion occur in
children under five years of age : —
In Edinburgh, 1925, 76 per cent. under five, 24 per cent. between 5 and 15. (p. 61 of Report.)
In Liverpool, 1916-1925, of 1,366 deaths, 65 per cent. were in children under age of 5 years. (p. 42 of Report.)
In Liverpool, 1925, 69 per cent. of deaths were under 5, and 24 per cent. between 5 and 10 years.
It is obvious that when, in seeking to prove the efficacy of immunisation, these two classes are lumped together and the total deaths among "immunised" and "non-immunised" given, the greater number of deaths are bound to be among the NONIMMUNISED.
IN JUDGING EVIDENCE AS TO DIMINISHED DEATH-RATES AMONG "SCHICK" IMMUNISED NO STATISTICS SHOULD BE ACCEPTED WHICH OMIT PARTICULARS AS TO AGE-GROUPING, BY WHICH SOME COMPARISON BETWEEN INOCULATED AND NON-INOCULATED CLASSES CAN BE SCIENTIFICALLY EFFECTED.
Even when the statistics show the age-grouping of the diphtheria cases, it must be remembered that the uninoculated class differs in other respects from the inoculated (stamina, general health, social conditions, etc.).
DR. A. BRADFORD HILL, one of the most respected statisticians in the medical profession, pointed out in articles in the Lancet in February and March, 1937, how fallacious conclusions are arrived at in regard to the protection afforded by inoculation. He showed that even if it was presumed that the inoculated groups and the uninoculated groups were equal in such characteristics as age, sex and duration of exposure to risk, it is possible that they were differentiated in other relevant ways DR HILL went on to say —
"Those who voluntarily come forward for inoculation may consist of individuals who also take other precautionary measures to avoid infection—e g the avoidance of theatres and cinemas during the epidemic period They may belong to a class higher in the social scale and be less exposed to the risk of infection thereby-e g by living in less crowded conditions or by being better nourished. In comparing the inoculated with the uninoculated we must always consider closely whether we are in fact comparing like with like— except in the one respect of inoculation ‘ (p 708)
3. ERRORS DUE TO NATURAL VARIATIONS IN INCIDENCE
In estimating any effect upon the incidence of diphtheria of any preventive measure it is necessary to take into account the curve of incidence over a large number of years both before and after its introduction, owing to the normal wide fluctuations of the disease apart from any form of treatment This has already been stressed in the quotations from DR FRIEDBERGER PROFESSOR TOPLEY and others (See pp 12 and 56 ante)
PROF ULRICH FRIEDEMANN of Berlin has also pointed out that —
"Diphtheria has a typical time curve with a constant ebb and flow It appears as an epidemic extending over some 30 years, disappears and then begins another period of 30 years."(The Lancet Aug 4th 1928 p 213)
The following letter from DR STEPHEN ROWLAND M O H for Northampton which appeared in the Lancet December 24th 1927 should be borne in mind in this connection He wrote —
"The mere fact of there being a lull in the number of notifications of diphtheria following immunization does not necessarily prove anything. During the summer I received a visit from a Swedish M.O.H., when, amongst other matters, we discussed diphtheria. He told me that it had almost disappeared from his town of late years and on my asking if it was due to toxin antitoxin immunization, my friend replied: ‘Certainly not. Whatever be the cause, it is not immunization, for I have not practised it and do not intend to do so, as I do not believe in it.’ Up to the time of writing we have had a very considerable fall in the number of notifications of diphtheria in Northampton and for some months it has apparently been almost absent from the town, there not having been a single case in a child of or under school age. Again, this happy state has not been brought about by toxin-antitoxin immunization, for it has never been attempted here (p 1366)
In his Annual Report for 1933, DR. STEPHEN ROWLAND again refers to the decline of diphtheria in Northampton without immunisation. (This will be found quoted on page 119, par. 3.)
According to A. R. SOUTHWOOD, M.D., M.S., writing in the Medical Journal of Australia, October 29th, 1932, the death-rate from diphtheria in South Australia fell from 249 per million living in 1921 to 3 per million living in 1930. He commented : —
"The rapid fall in incidence in South Australia from 1921 to 1930 would doubtless be quoted as favourable evidence if an extensive campaign of immunisation had been going on during that time. It is easy to see that misleading conclusions might be drawn from the consideration of statistics covering only a few years." (p. 536.)
As regards Sweden, a country which has remained practically without immunisation, in the Times (London), May 6th, 1938, it was stated : —
"Medical authorities are puzzled by the virtual disappearance of diphtheria from Sweden. The State Board of Health in its latest fortnightly report announces only one case in the whole population of over 6,000,000 people."
DR. VYNNE BORLAND, Medical Officer for Bethnal Green, in his Annual Report for 1934, stated that statistics—
"indicate that reduction in diphtheria incidence sometimes occurs irrespective of immunisation schemes and that this is markedly true of the great improvement in diphtheria mortality which has occurred during the past thirty-four years. Whether such improvements would be enhanced by immunisation is arguable."
At the annual meeting of the British Medical Association at Bournemouth in 1934 the President, DR. CARNWATH, was reported as saying : —
"It had been claimed that the fall in diphtheria mortality in New York had been due to wholesale immunization, but during the same period there had been a corresponding fall in London without this." (British Medical Journal. August 11th, 1934, p. 274.)
In Public Health Reports, May 5th, 1933, EDWARD A. LANE, M.D., M.P.H., suggested the influence of the larger, long-range annual variations in meteorological conditions as an explanation of the almost uniform decline in the mortality from diphtheria in all those American States for which statistics are available.
In an article entitled " Trends in the Prevalence of Diphtheria," which appeared in the Journal of infectious Diseases (Chicago) Vol. 58 (1936), ESCHSCHOLTZIA L. LUCIA and HILDA F. WELKE, of the Department of Hygiene, University of California, Berkeley, and the Department of Public Health, San Francisco, California, discuss the difficulty of presenting evidence in favour of serum-therapy or active immunisation on account of the lack of adequate data. They say : —
Because of this incompleteness of available statistics, it is impossible to determine how much of the downward trend of diphtheria mortality and morbidity has been due to the use of serum therapy and active immunization, and how much has been due to changes in population, environment, and in the disease itself.
"The statistics which are available are not sufficiently specific to show whether or not active immunization has caused a decline in morbidity. As in the case of mortality from diphtheria, advantage is being taken of a falling market." (p. 306.)
They came to the conclusion (see also p. 57), that : —
"The two medical procedures, passive and active immunization, can hardly be held responsible for the almost universal decline of diphtheria." (p. 307.)
In the Supplement to the Bulletin of the International Bureau of Public Hygiene (Paris), September, 1936, a report dealing with the problem of diphtheria in France states that : —
"In such conditions which present themselves frequently, it is difficult to state which part of the diminution in the number of cases is due to vaccination and which part results from spontaneous variations in the incidence."
4. Some eminent bacteriologists do not accept the statistical method when dealing with epidemics.
PROFESSOR MAJOR GREENWOOD, in his work, Epidemics and Crowd Diseases (Williams and Norgate, Ltd., London, 1935), remarks that " a respectable minority of epidemiologists, including men of great intelligence and wide experience, believe that the statistical method is of small value to the practical epidemiologist." (p. 17.)
In dealing with the artificial immunisation of man PROFESSOR GREENWOOD thinks that "a certain statistical test might lead to arithmetically overwhelming odds in favour of the inoculated, yet this a priori inference might be quite wrong. It might be that in some of the experiments neither inoculated nor uninoculated ran any serious risk at all; if in these groups there was a great majority of inoculated, the final summary would show a great advantage to them." (p. 84.)
He also points out that "Another fallacy of the same type, but not quite so obvious, is involved if comparison of attack-rates upon inoculated and uninoculated is made when the inoculation has been carried out during the course of an epidemic. The fallacy here is that the time risks of the two classes are unequal." "No data of inoculations performed during an epidemic are to be used unless sufficient details are given to enable one to allocate the time units of exposure to risk." (p. 85.)
Space precludes further quotation, but the reader interested in this aspect of the problem is strongly urged to consult PROFESSOR GREENWOOD’S masterly work.
SECTION
10
THE FALLACY OF THE THEORY OF IMMUNITY
THE TRUE CAUSE OF DIPHTHERIA
THE PREVENTION OF DIPHTHERIA
THE FALLACY OF THE THEORY OF IMMUNITY
The theory of immunity is based on the assumption that even a mild attack of the disease, produced by the inoculation of the toxin, will provoke a condition of " immunity" in the body which will protect it from further attack. It is believed that in both the naturally acquired and the artificially induced disease protection is brought about by the development of "antitoxin" in the blood of the individual.
The following facts are difficult to reconcile with this theory: —
1. QUAIN’S Dictionary of Medicine (1902) states: —
"One attack of diphtheria confers no prolonged immunity upon its subject. Even during convalescence the patient has been known to develop the disease afresh, and this may be repeated more than once."
2. DR. CLAUDE BUCHANAN KER, Medical Superintendent, City Hospital, Edinburgh, in A Manual of Fevers (1912), wrote: —
"Second attacks are quite common, many persons suffering twice, or even more frequently, from diphtheria." (p. 240.)
3. GOODALL and WASHBOURNE, in A Manual of Infectious Disease 1896), state:—
"it is uncertain how far one attack of this disease protects against a second. Certainly relapses and second attacks are not very rare. Some authors, indeed, consider that one attack predisposes to another. This is doubtful; but probably one attack confers little, if any, protection." (p. 116.)
4. L. A. GARCIA (Arch. Latino-Amer. de Pediatria, January, 1929), remarks that: —
"All physicians have seen cases of repeated diphtheria, and it is difficult to believe that the immunity which spontaneous diphtheria cannot give to the child may be produced by vaccination."
5. DR. C. W. HURR, M.O.H. for Holborn, reported in The Lancet, November 7th, 1925, the case of a boy who, two years after the three routine injections, developed diphtheria for the third time in his life. (p. 964.)
6. The following comment is made in the Bulletin of Hygiene for June, 1934, under the heading "Vital Statistics and Epidemiology": —
"[Diphtheria.] .—Repeated attacks are not unusual. Zischinsky has seen several examples of three or four attacks in the same child and one case in a child who had six attacks in 18 months. The second attack in several cases ended fatally."
7. DR. A. T. W. POWELL, M.O.H. for Walthamstow, issued a leaflet in 1935, in which, while recommending preventive inoculation, he said: —
"Second attacks of diphtheria are comparatively common."
8. In A Manual of Bacteriology (1911) by HEWLETT, it was stated on page 217:—
"Antitoxin formation probably plays little or no part in acquired immunity or even in recovery from infection. In diphtheria, for instance, antitoxin is not found until the disease has subsided."
9. Later confirmation of this is to be found in a statement by PROFESSOR JURGENS before the Berlin Medical Society. It was reported in the Lancet, March 14th, 1931 (p. 598), and read as follows: —
"[Diphtheria] antitoxin had never been found in the blood of diphtheria convalescents or in cases of diphtheria after death. There was, therefore, in his opinion, no certain proof of the value of immunization against diphtheria." (p. 598.)
10. According to the British Medical Journal, October 31st, 1936 (Epit. of curr. med. lit., p. 69), J. WUSTENBERG writes from the Robert Koch Institute in Berlin : —
"It has been noted that even after diphtheria has recurred more than once a child may still prove Schick-positive."
11. The following statement was made in the Medical Officer, October 30th, 1937 : —
"The older textbooks taught that diphtheria was one of the infections most likely to recur. This has long been known to be an error, but second attacks are not very infrequent and we have no grounds for believing that artificial means could give higher immunity than the natural disease." (p. 183.)
12. In a letter to the British Medical Journal, February 5th, 1938, DR. ALEXANDER JOE, of the City Hospital, Edinburgh, writes: —
"The plain fact is that second attacks of diphtheria are not uncommon, and this is not so widely appreciated as it might be. . . . A definite history of previous attacks should not be regarded as excluding the diagnosis of diphtheria. In several instances in my own experience the results of such an assumption have been serious." (p. 305.)
13. PROFESSOR W. W. C. TOPLEY, in An Outline of Immunity (1933), states that as regards active immunisation:—
"The only way of dealing with this question in such a book is by a frank admission of our inability to answer it satisfactorily."
14. MR. J. E. R. MCDONAGH, in his Nature of Disease Journal (Vol. I, 1932, p. 69), maintains:—
"The whole subject of immunity is built upon an entirely false basis, and in many instances it would be better to treat the symptoms and let the cycle run its normal course than to prevent infection with a so-called ‘immuno-agent,’ which at the very best can produce no more than temporary immunity."
He points out in Vol. II, 1933 (p. 192), that : —
Every infection carries with it the weapons which are ultimately to destroy it "; and warns us that their action "may be seriously interfered with by the production of man-made milder infections."
ANCIENT BELIEF
The belief that a close relationship exists between epidemic diseases and bad sanitation and lack of hygiene generally was taught by HIPPOCRATES, the father of medicine, and held the field for two thousand years.
Known as the " miasmatic " theory, it was not until the advent of the erroneous Pasteurian doctrines towards the end of the last century that it became temporarily obscured.
SYDENHAM, the "English Hippocrates," elaborated it in the 17th century, and even as late as 1894 it was maintained by DR. CHARLES CREIGHTON in his classical History of Epidemics in Great Britain.
FAILURE OF MODERN THEORIES
Though disregarded, this theory has never been superseded, and in spite of 50 years’ research by believers in the Pasteurian "germ" origin of disease, none of the modern theories, as DR. C. A. GILL admits in his work, The Genesis of Epidemics and the Natural History of Disease, can claim to provide an adequate explanation of the cause of epidemics [The nearest approach to a rational theory of the basis of epidemics is to be found in the works of J. E. R. MCDONAGH, F.R.C.S., notably in The Nature of Disease Journal, Vol. II (pp. 149, 159), and The Common Cold and Influenza (Heinemann, 1986, p. 79)].
As a leading article in the Times of August 13th, 1930, pointed out : —
"The nature of these and other variations has exercised the minds of physicians and bacteriologists during many years, but it cannot be said that any very clear views about them have been formulated."
CORROBORATION OF ANCIENT BELIEF
In a paper he read before a branch of the British Medical Association at Maidstone on October 25th, 1861, DR. WILLIAM CARR declared : —
"All my carefully conducted inquiries induce me to believe that the disease comes from drain-poison. All the cases into which I could fully inquire have brought conviction to my mind that there is a direct law of sequence in some peculiar conditions of atmosphere between diphtheria and bad drainage." (Brit. Med. Jour., Dec. 7th, 1861, p. 607.)
In the discussion which followed, DR. MONCETON enlarged upon this conception, stating his impression that infection
"arose from what might be called an error in nature’s destructive assimilation of refuse matter. Effete animal and vegetable organisms were intended to decay back to the inorganic world as harmlessly as they emanated from it; but by thermal, electric, or some other perturbation, leaves, vegetables, animal matter, and sewage might at any time be evolving in the process of decay abnormal and damaging products, and this over an infinitely extended area." (Ibid.)
BeCHAMP’S teaching regarding the function of microzymas, together with modern knowledge regarding the chemistry of colloids, supply the connecting links between the extraordinarily accurate conclusions based upon long and painstaking observation (which we see were held by medical scientists before the misleading teachings of PASTEUR and his satellites of the laboratory cast their paralysing spell over medical thought) and a complete technical understanding of the problem which the intellect demands. But a detailed discussion of this subject lies outside the scope of this pamphlet.
The connection between diphtheria and sewage was again emphasised in 1894 in QUAIN’S Dictionary of Medicine as follows: —
"There is no doubt that exposure to sewage emanation is a fruitful source of diphtheria . . . the statistics of the association between the two are very positive."
PARKES and KENWOOD, in the 1907 edition of Hygiene and Public Health, say: —
"Faulty sanitary surroundings (drainage and health nuisances) tend to the production of diphtheria in the same way, namely, by engendering a morbid condition of the tonsils favourable to the growth of the diphtheria contagion if implanted thereon."
This clearly indicates that an antecedent morbid change in the "soil" is necessary before any so-called diphtheria germ can grow therein; thus establishing that the latter is not the true cause of the disease. (See pp. 6 and 7, ante.)
RECENT CONFIRMATION
DR. AUSTIN PRIESTMAN, M.O.H. for Folkestone, writing in the Medical World, February 6th, 1931, reported that investigation shows in interesting and conclusive fashion the definite effect of school buildings, their construction and sanitation, on the spread of diphtheria. The highest incidence was observed in those schools where sanitation is most deficient and ventilation and lighting the least satisfactory. The brightest and airiest school showed the lowest incidence, and the incidence throughout all the schools placed them in exact order of sanitary virtue."
"Moreover, the incidence indicated the schools where malnutrition in the children is most conspicuous." (p. 627.)
It is of interest to note that SIR ARTHUR NEWSHOLME " correlated diphtheria epidemics in England, and many other countries, with deficient rainfall" (see Epidemic Diphtheria, London, 1898), and that J. S. ANDERSON, F. C. HAPPOLD, J. W. McLEOD and J. G. THOMSON, in an article from which the above sentence is quoted and which appeared in the Lancet, January 19th, 1935 (p. 170), admitted that recent experience inclined them to the view that "there may well be something in NEWSHOLME’S theory." (See also: EDWARD A. LANE, M.D., M.P.H., p. 99 ante.)
This theory fits in very well with the statement in the Medical Echo, Vol. 8, No. 29 (Annals of the Picket-Thomson Research Laboratory, October, 1929), regarding the genesis of Follicular Tonsillitis, a disease not far removed from diphtheria, as is shown by the vast number of cases of diphtheria which, sent to hospital by doctors, are re-diagnosed as tonsillitis after admission (see p. 94 ante). The statement reads: —
"There is no question that the disease is contagious, and there are good grounds for believing that air contaminated by sewer gas or rubbish heaps may be a source of infection, though bacteriological evidence is difficult to obtain."
According to T. J. NICHOLL, F.R.C.S.I., Assistant M.O.H. for Dover :—
"The causes which predispose a person to infection are : —
(a) Damp atmosphere, which lowers the vitality of the upper respiratory tract.
(b) An unhealthy condition of the tonsils and mucous membrane of the naso-pharynx is a very suitable soil on which the bacillus may thrive.
(c) The debilitating effects of other infectious disease, such as measles, scarlet fever, whooping cough, and mumps." (The Journal of Clinical Research, April, 1934, p. 60.)
The importance of the factors involved under the foregoing heading (b) lies in the scientifically established observation that it is the medium or soil which determines whether or no the organism can (1) survive in the tissues, and (2) produce harmful toxins therein.
1. DR. J. E. MCCARTNEY pointed out in a paper before the Section of Epidemiology of the Royal Society of Medicine in 1928 that carriers invariably present some abnormal condition of the upper respiratory tract, although they may appear to be healthy people; for, he stated, "the organisms are able to live in the respiratory passages not upon living tissues, but’ upon the products of the inflammatory reaction and the excreta of the consistent rhinorrhcea." (The Journal of Clinical Research, Vol. XIV, No. 2, April 1928, p. 69; my italics.)
2. S. GURNEY DIXON, M.A., M.D., points out in his book, The Transmutation of Bacteria (Cambridge University Press, 1919, p. 90) that in the case of some organisms—for example, "Bacillus diphtheriae (THEOBALD SMITH 1899, FIshER 1909)—toxins are formed in a culture only if the amount of sugar is very small—not more than a ‘ trace ‘."
When once the principles involved in the causation of diphtheria are grasped, it will be realised how futile, unscientific and anti-social are all attempts at artificial immunisation.
As DR. JAMES WHEATLEY, in his presidential address to the Society of Medical Officers of Health in October, 1927, stated: —
"If disease is looked upon as an unmitigated evil, to be got rid of at all costs, and by every means available, then I think we are only taking a very partial and one-sided view that in the long run will lead to disaster.
If, on the other hand, disease is looked upon generally as an indication of something wrong in our mode of life, that should be remedied, and the investigation into disease is looked upon as one of the most valuable means of determining the laws of healthy living, then we have a broad conception on which real and lasting health ‘work can be based.
"It is not sufficient to get rid of disease; it must be got rid of in the right way; otherwise the balance of good and evil may be on the wrong side." (Public Health, November, 1927, p. 43.)
As an instance of wrong means, it is only necessary to glance at the methods of propaganda commonly adopted by both central and local health authorities.
HOW HEALTH DEPARTMENTS INSTIL FEAR OF DISEASE.
In the Medical Officer, January 25th, 1936, DR. E. A. UNDERWOOD, M.O.H. for Shoreditch, declared: —
"Fear is the greatest of all propagandists. During the early part of the present year (1935) diphtheria was extremely prevalent in many parts of the country, and reports in the press diffused knowledge of the dangers of the disease" (not, be it noted, of the dangers of inoculation). "The result of this knowledge, which was stimulated by the personal efforts of members of the health department staff, was a very marked increase in the number of children who attended for immunisation." (p. 38; my italics.)
FEAR, NOT REASON, HAS MARKED THE OFFICIAL PROPAGANDA IN FAVOUR OF IMMUNISING INOCULATIONS AGAINST DIPHTHERIA.
The main preventive measures which alone can be successful in eliminating diphtheria epidemics " embrace wholesome food, hygienic clothing, a sufficiency of fresh air and an adequate elimination of waste products," to quote the words of J. E. R. MCDONAGH which refer to infections in general. (Nature of Disease Journal, Vol. 2, 1933, p. 193.)
It is obvious that the reforms, educational, social, sanitary, necessary to bring about this desirable state of things will be indefinitely delayed and thwarted if the current orthodox belief is allowed to gain ground that the unpleasant results of their neglect, namely, epidemic diseases, can be more easily and cheaply avoided by inoculating helpless children [In this connection the statement by MAJOR GREENWOOD, D.Sc., F.R.C.P., F.R.S., quoted on page 123, post, is particularly apposite.]
This is the main reason why this type of "preventive medicine " is so strenuously supported by vested interest, for not only are vast fortunes derived from the manufacture of the various immunising materials, but, what is even more important, all those powerful interests which are directly or indirectly adversely affected by the march of social progress stand to gain by the promulgation and adoption of this delusion which is being thrust upon the public.
We may fitly conclude this survey of the important problem of artificial immunisation against diphtheria in the words of JAMES GORDON CUMMING, M.D., D.P.H.; in an article in the Journal of the American Medical Association, March 4th, 1922, he wrote:—
"The eradication of diphtheria will not come through the serum treatment of patients, by the immunization of the well, or through the accurate clinical and laboratory diagnosis of the case and the carrier followed by quarantine; rather it will be attained through the mass sanitary protection of the populace subconsciously practised by the people at all times." (p. 632.)
We shall find no more practical advice than that given by DR. AUSTIN PRIESTMAN, Medical Officer of Health for Folkestone, when, in an article on "Epidemic Diphtheria " in the Medical World, February 6th, 1931, he declared:
"Rather than attempt wholesale immunisation by artificial means we should adopt the same plan of campaign against bacillus diphtheriae as we adopted against the bacillus of tuberculosis—namely, provide better ventilated, better lighted and better equipped schools, and feed all children who need feeding.’ (p. 627.)
DR. PRIESTMAN re-emphasised his contention in the Medical Officer, March 9th, 1935, when, in reporting his unfavourable experiences with immunisation, [see p50, par16] he wrote: —
"It is safer to help man and his resistance through the healing channels of work and food and recreation, and to leave to Nature an immunisation which she will give, perhaps more slowly that we wish, but more efficiently and with a more true economy." (p. 99.)
As SIR WILLIAM ARBUTHNOT LANE declared in the February, 1937, issue of New Health, of which he is Consulting Editor:—
"It is much better to endeavour to create a natural immunity by fostering good health than by attempting to induce an artificial immunity by doubtful vaccines."
SECTION
11
SUFFERING TO ANIMALS INVOLVED IN THE MANUFACTURE AND TESTING OF SERA
The cruelty to animals involved in the preparation of antitoxin and immunising mixtures falls under four heads: —
(1) As regards the horses (or other animals) used in the manufacture of serum.
(2) As regards the guinea-pigs used for standardising the toxin.
(3) As regards the guinea-pigs used for standardising the serum obtained from the horse
(or other animal).
(4). As regards testing for organisms in throat swabs.
For the production of serum horses are injected with gradually increasing doses of toxin, or toxoid, two or three times a week.
The following description is quoted from HEWLETT and MCINTOSH’S A Manual of Bacteriology (CHURCHILL, 1932):
"Individual horses vary in their susceptibility to the toxin, so that care has to be exercised with the earlier injections. The injections are given subcutaneously over the shoulder, and produce local swelling with some rise of temperature and general disturbance, lasting two or three days. When this has passed away the inoculation is repeated, a larger dose being administered provided the reaction due to the former was not too severe."(p. 294.)
"A horse to be of value should after three months’ treatment yield an antitoxic serum containing not less than 300 units per cubic centimetre. The required potency having been ascertained, as shown by the test described below, the horse is bled with aseptic precautions, the blood is allowed to coagulate, and the serum is separated and filled into sterile bottles." (p. 295.)
"Wadsworth (1927) gives the detailed record of a horse which in 9 years gave 161 bleedings of about 8 litres." (A System of Bacteriology. 1929, p. 356.)
In some cases the blood corpuscles are re-injected into the horse,
"which is thereby deprived only of plasma and is consequently able to withstand more frequent and larger bleedings." (A Manual of Bacteriology, p. 295.)
In the Medical Research Council’s Report on diphtheria (1923) it is stated:—
"Among the ill-effects that may follow toxin injections, the most severe are paralysis, and death of the horse with fatty degeneration of the heart and degenerative changes in the kidney. A chronic malady sometimes supervenes in animals which have undergone for some years continuous courses of antitoxin-production. . . . The animal soon becomes ill and eventually dies with amyloid degeneration of the spleen and liver, and with hepatic and peritoneal hemorrhages." "Even with the greatest precautions a certain proportion of animals fall victims to acute toxaemia." (pp. 131 and 134.)
Here is a description of the effects of the injection of toxin on horses, extracted from a volume entitled Experimental Bacteriology by DR. W. KOLLE and DR. H. HETSCH, of Frankfort, the English version [GEORGE ALLEN & UNWIN, LTD., London, 1934] of which is edited by DR. JOHN EYRE, Director of the Bacteriological Department, Guy’s Hospital. In Chap. XII we may read : —
"In order that the animals even when restless may do as little harm as possible by kicking, they are put in the stand which consists of four padded walls which are fastened by iron rails to strong cemented wooden posts. The anterior and posterior walls at the same time act as doors. If large quantities of liquid are to be injected, it is advisable to suspend the animals by means of slings so that the acute reaction may not result in an accident. If the horse is unconscious after the injection, it may then be slowly lowered to the ground without being injured. The suspension apparatus can be worked with a set of pulleys fastened to a strong beam.
"Further phenomena are exhibited at the close of the injection period, namely: Restlessness, disinclination to eat, shivering, rise in temperature, diarrhoea, and oedematous swellings of the extremities, particularly of the joints. These reactions, especially at the commencement of immunisation, may continue over two weeks, but as the degree of immunity is increased their duration will be less, finally amounting only to three to five days. Nevertheless, it is well to grant the animals some respite between the several injections, especially when the weekly weighings indicate a persistent decline.
"Anaphylaxis, due to the continued parenteral introduction of bacterial proteins, plays a considerable part in causing these acute reactions; in particular, acute cases resulting in death are for the most part to be attributed to the action of anaphylatoxins.
"If an animal has concluded its last period of immunisation and is no longer suited for further treatment, it is sometimes advisable to bleed it completely."
In Recent Advances in Vaccine and Serum Therapy (1934), we learn that some reactions in the horse are an advantage to the manufacturer, however painful to the animal, for—
"Ramon noted an increase in the amount of antitoxin in the blood of horses when sterile abscesses happened to form at the site of the inoculation, and from this observation he was led to produce artificial sterile abscesses by mixing the toxin with a tapioca preparation." (p. 2.)
2. In HEWLETT’S A Manual of Bacteriology (1932) it is stated in regard to standardisation of toxin (p. 297) that—
(a) The minimum lethal dose of a toxin is estimated by finding the amount which injected into a series of guinea-pigs kills on the fourth or fifth day. (Those that die after this period do not count. M. B. B.)
(b). The least amount of toxin which, mixed with a unit amount of antitoxin (standard) just kills a guinea-pig on the fourth or fifth day is known as the L + dose, and is the amount of the test toxin now usually employed for standardising each fresh batch of antitoxin. (See 3 (b) post.)
In A System of Bacteriology (Medical Research Council, 1929, Vol. V, p. 90), we may read:—
"By the end of 24 hours after inoculation the animal usually manifests symptoms of acute illness. It will be found cowering in a corner of its cage, with coat ruffled and with definite dyspnoea. It is cold to the touch . . . the weight diminishes rapidly up to the moment of death in about 4 days. A dose of diphtheria culture or toxin which will kill in this time is spoken of as the ‘minimum lethal dose’ (M.L.D.). Multiples of this quantity will kill guinea-pigs in as short a time as 24 hours with symptoms correspondingly violent and acute."
"When the culture is not in its most virulent state or the dose is small, the animal may survive, for a week, or even much longer, and finally succumb in a state of marasmus. The local lesion, at first soft, becomes indurated; necrosis sets in and the whole affected area may slough and leave a slowly healing granulating wound."
The pathological condition produced by the injection into the guinea pig [Further slight indication of the suffering involved may be gained from the description of the illness of five children, two of whom died, resulting from the accidental inoculation of diphtheria toxin intended for animal experimentation in place of an immunising mixture. The tragedy has already been referred to on page 64, ante; the "severe symptoms" noted were "fever, swelling of their arms with unusual pain."] is described in HEWLETT’s A Manual of Bacteriology (1932), as follows:—
"At the site of the inoculation haemorrhagic oedema forms, haemorrhages occur in the serous membranes, and especially in the adrenals, while the renal epithelium and the liver cells undergo cloudy degeneration." (p. 290.)
"The unit of diphtheria antitoxin may for practical purposes be defined as an amount which neutralizes approximately 100 M.L.D,s of diphtheria toxin for the guinea-pig."
Note: Standardisation of antitoxic serum is effected by two methods: —direct and indirect.
(a) In the first, the amount of serum which, when mixed with the M.L.D. of toxin and injected into a guinea-pig, is sufficient to prevent death, is ascertained. The number of units contained is then calculated. [The reason for the general abandonment of the method of standardisation given under (a) is given in Evans’ Journal (New Series), Vol. 4, No. 2 (Nov., 1938), as follows:— "In all biological tests very many different factors have to be taken into consideration, the chief being animal variation. There is always in the living animal variation in susceptibility to any condition, this variation often being very inconsistent, altering from day to day, season to season, and according to the conditions under which the animals are fed and kept. The result of the summation of such variable factors alone renders it impossible accurately to standardise a preparation in terms of units as dog, cat, pigeon units, etc., as was once, and on occasion is still, practised." (p. 54.)]
(b) In the second, the amount of serum which, when mixed with the L + dose of toxin (previously described), protects a standard guinea-pig, is used as the basis of calculation.
In either method the antitoxic serum is injected in graduated dilutions into a whole series of guinea-pigs and those in whom the antitoxin is not sufficient to neutralise the toxin succumb in varying periods as previously described.
4. In addition to the suffering involved in the above procedures, further inoculations into animals are frequently performed in the course of tests of the virulence of organisms found to be present in the throats of patients. After the specimen from a throat-swab has been incubated on a special medium, in a test-tube,
"The whole of a young serum slope [The culture grown upon the sloping surface of the culture-medium in a test-tube] is emulsified in saline and injected subcutaneously into a 250 grm. guinea-pig. If the strain be virulent, death will usually ensue in one or two days with the characteristic post-mortem appearances." (A Manual of Bacteriology, HEWLETT and MCINTOSH, 1932, p. 311.)
The sufferings which precede death, and the post-mortem changes to be observed, have been described under heading 2 on the previous page.
In the Ministry of Health’s Report on Diphtheria, No. 10 (p.80), a different method is described in which the culture to be tested is injected "intra-cutaneously," i.e., into the abdominal skin of a guinea-pig which has previously been depilated "preferably by pulling the hair out."
This, they inform us, can be done "with probably less pain than is associated with the prolonged irritation which, at times, follows the application of depilatory barium sulphide paste." Additional guinea-pigs, previously injected intracardially (in the heart) with antitoxin, are used as controls; these latter animals are employed over and over again.
SECTION 12.
WHAT EMINENT DOCTORS THINK ABOUT INOCULATION
The following quotations are without exception from the writings of Medical Officers of Health and other authorities of unquestioned distinction in the domain of medical science.
They must be regarded as the considered opinions of doctors whose position in public office and experience in public health matters entitle them to a serious and respectful hearing at the hands of their colleagues throughout the profession.
Many of the quotations have already appeared in preceding sections of this pamphlet, but it is thought a useful purpose will have been served by gathering them together in one chapter.
‘The eradication of diphtheria will not come through the serum treatment of patients, by the immunisation of the well, or through the accurate clinical and laboratory diagnosis of the case and the carrier followed by quarantine; rather it will be attained through the mass sanitary protection of the populace subconsciously practised by the people at all times." (J.A.M.A., March 4th, 1922, p. 632.)
2. DR. JAMES WHEATLEY, in presidential address to the Society of Medical Officers of Health, in October, 1927, stated:
"If disease is looked upon as an unmitigated evil, to be got rid of at all costs, and by every, means available, then I think we are only taking a very partial and one-sided view that in the long run will lead to disaster.
"It is not sufficient to get rid of disease, it must be got rid of in the right way; otherwise the balance of good and evil may be on the wrong side.
"One often hears a statement such as this . . . the Schick test should be applied throughout the land and followed up by immunisatron. My contention is that the problem is a much more complicated one, and that before deciding upon such a course the balance of good and evil should be carefully weighed (Public Health, November, 1927, p. 43.)
3. DR. STEPHEN ROWLAND, Medical Officer for Northampton :—
"The mere fact of there being a lull in the number of notifications of diphtheria following immunisation does not necessarily prove anything."
Commenting on the almost entire absence of the disease from Northampton, he wrote: —
"This happy state has not been brought about by toxin-antitoxin immunisation, for it has never been attempted here." (The Lancet, December 24th, 1927, p. 1366.)
In his Annual Report for 1933, he wrote:—
"Immunisation has not been practised in this town, the marked decrease in diphtheria during recent years having come about without any artificial means; it is merely a phase in the periodicity or wave of the disease, a periodicity not confined to diphtheria but seen in other infectious diseases . . . Had we practised immunisation and ‘protected,’ say, two thousand children of different ages during the last few years, we could have pointed to 1933 as a triumph of immunisation, but with how much truth?
(Quoted in The Medical Officer, March 9th, 1935, p. 95.)
4. DR. STEPHEN ROWLAND also quotes a Swedish M.O.H. who, when asked if the disappearance of diphtheria from his town could be attributed to immunisation, replied : —
"Certainly not. Whatever be the cause, it is not immunisation, for I have not practised it and do not intend to do so, as I do not believe in it." (The Lancet, December 24th, 1927, p. 1366.)
"All physicians have seen cases of repeated diphtheria, and it is difficult to believe that the immunity which spontaneous diphtheria cannot give to the child can be produced by vaccination." (Arch. Latino-Amer. de Pediatria, January, 1929.)
6. J. F. C. HASLAM, M.D., M.R.C.P., D.P.H., author of Recent Advances in Preventive Medicine (1930), writes in regard to the value of immunisation : —
"None of the published figures of results in children, of which I am aware, is valid proof of this advance" (p. 293). However, he admits: "Be the ascertained facts what they may and the final issue what it may, a health department will probably get away with it, if it comes before the public with a fresh method of prevention" (p. 296).
7. PROFESSOR JURGENS, discussing the value of immunisation before the Berlin Medical Society; —
"Antitoxin had never been found in the blood of diphtheria convalescents or in cases of diphtheria after death. There was, therefore, in his opinion, no certain proof of the value of immunisation against diphtheria." (The Lancet, March 14th, 1931, p. 598.)
8. DR. AUSTIN PRIESTMAN, Medical Officer for Folkestone, advised:—
"Rather than attempt wholesale immunisation by means we should adopt the same plan of campaign bacillus diphtheria as we adopted against the culosis—namely, provide better ventilated, better lighted better equipped schools and feed all children who feeding." (Medical World, February 6th, 1931, p. 627.
9. DR. FRIEDBERGER, in an address before the Berlin Society: —
"As regards active immunisation against diphtheria its introduction had not caused any change in the occurence of epidemics, and that all the statistics as to its success, mainly emanated from American sources, were based on erroneous conclusion that the decline in the incidence diphtheria was due to immunisation, whereas the immunisation was being carried out when the disease was showing a tendency to abate." (The Lancet, March 14th, 1931, p. 598)
10. J. E. R. MCDONAGH, F.R.C.S, the eminent bacteriologist:—.
"The whole subject of immunity is built upon an entirely false basis." (Nature of Disease Journal, Vol. I, 1932, p. 69.)
Every infection carries with it the weapons which are ultimately to destroy it." He warns us that the action of these weapons " may be seriously interfered with by the of man-made milder infections." (Nature of Disease Journal, Vol. II, 1933, p. 192.)
11. DR. C. BANKS, Medical Officer for Nottingham, in his Annual Report for 1933:—
"I have not considered it desirable to start a towards general immunisation against diphtheria in a community which has shown itself so unwilling to avail itself of vaccination against smallpox." (Quoted in The Medical Officer, March 9th, 1935, p. 95.
12. DR. VYNNE BORLAND, Medical Officer for Bethnal Green, his Annual Report for 1934, stated that statistics—
"indicate that reduction in diphtheria incidence occurs irrespective of immunisation schemes and that markedly true of the great improvement in diphtheria mortality which has occurred during the past thirty-four years. Whether such improvements would be enhanced by immunisation is arguable.
In the absence of substantial proof . . is the proper line of action to launch a vigorous immunisation campaign (anything less would appear to be of little value) or to spend the money and labour involved towards other more tangible public health activities?
" In all the circumstances the weight of evidence seems to me to be decidedly in favour of the second of the two courses indicated above."
13. Under the heading "The Public Health Department: From the Desk of a " M.O.H.’," a medical officer writes:—
"So far as the claims made on behalf of the immunising campaign are concerned, I cannot help feeling that, for the present, at any rate, in this country, it may be dangerous to exaggerate." (Municipal Engineering, Sanitary Record and Municipal Motor, January 10th, 1935.)
14. DR. C. V. DINGLE, Medical Officer for Middlesbrough, reported to the, Health Committee of that town : —
"I came to the conclusion that it was too much in the experimental stage for me to recommend it. It has its drawbacks. The child has to have three injections which may set up some local disturbance, which may be mild or severe, and it takes a month or more for protection to be established I cannot advise you to go in for a wholesale public immunisation in Middlesbrough." (Yorkshire Post, January 16th, 1935.)
15. D. M. CAMERON, M.B., B.Ch.
" Scarlet fever and diphtheria are questionable as regards the value of prophylaxis, and reactions are not sufficiently regarded by enthusiasts. Before the country is stampeded into mass immunisation this problem of side effects should be most thoroughly gone into, e.g., anaphylaxis with serum, encephalitis with vaccination." (The Pharmaceutical Journal, February 2nd, 1935, p. 117.)
16. C. KILLICK MILLARD, M.D., D.Sc., (then) Medical Officer for Leicester, in a Report [see page 45, ante] to the Health Committee of that city : —
" In view of the facts and considerations adduced above [in the report] I feel that I cannot recommend the Health Committee of Leicester City Council to take any action at present in the direction of encouraging inoculation of the general public. I think it would be wise to wait until there is a little more certainty that good and not harm is likely to result."
"Taking the five years 1929-1933, the average diphtheria mortality figure for Leicester comes out at three per 100,000. The figure for England and Wales was seven. That for Birmingham was SIX ifl spite of the fact that 45,000 children had been inoculated." (The Medical Officer March 9th, 1935 p 96)
Later in his Annual Retort (for 1934) DR K1LLICK MILLARD added —
"Although the above report and its conclusions and recommendations run counter to the present day tendency—there being a definite wave of enthusiasm in. favour of inoculation— your Medical Officer has received sufficient support and approval from other Medical Officers of Health to show that there are two sides to this question
"On the surface it seems unlikely that a measure so perpetually expensive m time labour and money should yield satisfaction."
It is safer to help man and his resistance through the healing channels of work and food and recreation, and to leave to Nature an immunisation which she will give, perhaps more slowly than we wish, but more efficiently and with a more true economy." (The Medical Officer, March 9th, 1935, p. 99.)
18. DR. MODLIN, Chairman of the Health Committee of the Sunderland Town Council, at a meeting of the Finance Committee,
"opposed a Labour amendment to reinsert in the estimates £500 for immunisation against diphtheria. He said the system was not infallible and many expert medical men were against it. It was impossible to obtain the general consent of parents and unless 80 per cent. consented it was useless; £500 would be merely touching the fringe of the question. ‘The cost,’ he said, ‘is 10s. per child, treatment takes five months to become effective, and during that time you are increasing the, danger because you have increased the number of carriers of diphtheria germs ‘." (Manchester Guardian, March 13th, 1935.)
19. DR. W. F. BETENSON, School Medical Officer, Breconshire : —
"Asked for his opinion on the matter [a scheme for the immunisation of school children] Dr. Betenson said he did not agree with the suggestion. So far there were only three cases notifiable. If they decided on immunising school children there was a danger of them conveying the bacilli to children who were not iminunised, and they might easily catch diphtheria." (Hereford Times, April 6th, 1935.)
20. MAJOR GREENWOOD, D.Sc., F.R.C.P., F.R.S., makes the following significant statement in Epidemics and Crowd Diseases (1935, p. 75):—
"It is a great deal better to provide clean houses and food than to pre-immunise people against the possible consequences of dirty houses and food, leaving environmental conditions alone. It is fortunate for the world that pre-immunisation against the typhoid group was not discovered in the days of laisser faire; had it been, many more thousands would have died of typhoid than actually did. Eighty years ago it would have been hard to persuade the possessing classes to spend money on safeguarding water supplies if so cheap an alternative method of protection could have been provided."
21. THE MEDICAL OFFICER OF HEALTH FOR WEMBLEY, in his Annual Report for 1984 : —
"In recent years the incidence of diphtheria has shown a tendency to decrease, and one cannot be certain that the alleged improvement in the mortality rate is really due to the immunisation, especially as the larger towns, where nothing has been attempted, show a precisely similar drop in the number of deaths." (Wembley News, August 23rd, 1935.)
22. DR. HARRIS, Minister for Health in Victoria, Australia:—
"You can state anywhere, at any time, that I did say publicly that on no account whatever would I risk my own children’s lives by having them immunised."
(The Voice, Hobart, Tasmania, May 15th, 1936.)
23. J. WÜSTENBERG, a German medical scientist, is quoted in the British Medical Journal, October 3 1st, 1936, as stating: —
"Although wholesale immunization against diphtheria has been undertaken in Germany during the past few years, opinions are yet divided about its value.
"It would seem that there is at present no criterion by which the degree of protection against diphtheria afforded by active immunization can be gauged." (Epitome of Current Medical Literature, p. 69.)
24. DR. E. ANGUS JOHNSON, Medical Officer of Health for Adelaide, S. Australia : —
"Dr. Johnson says that he was, therefore, still of the opinion that Adelaide Board of Health should not recommend, for the present at any rate, general immunisation, as a lot had yet to be learnt concerning immunisation and its effects on the community in general." (The Western Australian, July 24th, 1937.)
25. DR. T. B. HILL SCOTT, Medical Officer of Health for Antrim Rural District: —
"In conclusion I wish to congratulate you [the Antrim Rural District Council] on the stand you have taken and your refusal to be rushed. You evidently feel very much as I do myself, and I have every sympathy with you. Like myself, you are doubters, and before experimenting in such a vitally important matter, you are inclined to wait for more exact and convincing information, if such be forthcoming." (The Belfast Newsletter, October 19th, 1937.)
26. The Medical Times, November, 1937, in its editorial, stated : —
"We believe this is the only medical journal that has warned its readers against the risks attending immunisation against disease. To-day we have prophylactic sera or vaccines against such diseases as the common cold, influenza, typhoid and so on. Immunisation against diphtheria is one of the latest, we might almost say one of the latest crazes. At any rate, we again wish to sound a note of warning against it. We really know far too little about the actual results of immunisation to warrant us meantime in adopting such measures. Unfortunately deaths following immunisation have been reported from time to time. This should make us go very cautiously."
27. C. C. OKELL, M.C., M.A., Sc.D., F.R.C.P., late Bacteriologist, University College Hospital, writing under the caption, Grains and Scruples," in the Lancet, January 1st, 1938, stated : —
"That diphtheria can be prevented by immunisation no more implies a command to immunise people than the fact that nitric acid and glycerine make an explosive mixture implies a command to blow up our neighbours. Yet the immunisation of the masses is undertaken with almost religious fervour. The enthusiast rarely stopped to wonder where it would all finish or whether- the fulsome promises made to the public in the form of ‘ propaganda’ would ever be honoured. (p. 48.)
"Those who have had to take detailed notice of the immunisation accidents of the past few years know that to get the truth of what really went wrong generally calls for the resources of something like a secret service. (p. 48.)
" Immunisation surely should remain a matter of private, not of public, venture—a question for the individual to decide on personal grounds and in terms of his own risks, fears and prejudices." (p. 49.)
ADVICE GIVEN BY THE MINISTRY OF HEALTH
The Medical Officer, October 5th, 1935, contained letters from DR. A. D. SYMONS, Medical Officer of Health for Shrewsbury, and DR. G. K. BOWES, Medical Officer of Health for Bedford, in which the writers referred to the extremely low incidence of diphtheria in their respective boroughs in spite of very little immunisation, and to the undesirabiity of pushing diphtheria immunisation against the wishes of the inhabitants.
In the following week’s issue of the Medical Officer (October 12th, 1935), DR. F. A. BELAM, Medical Officer of Health for Guild-ford, contributed a remarkable letter in which he reported the outcome of an interview he had had with one of the medical officers of the Ministry of Health.
In his letter, DR. BELAM stated that the advice which he received from this officer of the Ministry, and which he subsequently reported to his committee, was as follows : —
1. ADVERTISEMENT. The Ministry deprecate very strongly any advertisement or concentrated push directed towards persuading parents to get their children immunised. The reason for this is that they wish parents to exercise their own free will in this matter, and bring their children voluntarily for immunisation, should they desire it. The Ministry consider that the demand for immunisation should come from the public, and that it is very wrong to attempt to force people to get their children immunised. If parents ask voluntarily for immunisation, they will be told exactly what immunisation does and also what it does not do. Should any reaction in the shape of feverishness or anything else take place, it cannot then be laid to the fault of the authority.
2. No special immunisation clinic should be established.
DR. BELAM added that his council concurred with this advice and as a consequence he had received up to date applications from parents of only three children for immunisation, since the previous February.
He further stated that, like DR. SYMONS, he had had no outbreak of diphtheria since 1929 and he did not feel disposed to start any scare, "particularly in view of the deprecation of the Ministry of any advertisement whatever."
It will be noticed that the foregoing advice is in marked contrast to what is usually assumed to be the official view of the Ministry of Health. It seems significant, however, that although wide publicity has been given to Dr. Belam’s letter, no retraction
[Home]