AUTISM: THE EVOLUTION OF A DISEASE
by Bryan Jepson,
MD
Thoughtful House
Presented at the National Autism Association conference.
I want to start by talking about how I got here. This is my biography:
• Graduated from University of Utah Medical School in 1995
• Completed residency in emergency medicine in 1998
• Began career as ER physician in Colorado Springs in 1998
• Board certified in emergency medicine 1999
If you scan through the list, you'll see that there's nothing in there about
autism. I am an emergency medicine-trained
physician--very mainstream, very traditional. In 1998 I
finished residency and started my career, happy to become a very
anonymous ER doctor who completed his shift and went
home to spend time with his family.
For a long time, everything went as planned. In 1998 my second son Aaron was
born. You can see in his toddler pictures that he was very well
connected, very happy, and
he had great eye contact. He was a normally-developing kid. We had no reason to
suspect that there was anything wrong with him. In fact, my older son had
more of the characteristics we associate with autism.
He was very colicky and very sensitive to sound and
light when he was a baby. So, Aaron was a real pleasure. In a picture of Aaron
after his third birthday, you can see that he was a different child. He
no longer had any eye contact, he was pale, he did not
appear happy or healthy, and he was no longer
connected. Although we were concerned about him, we didn’t suspect autism. Our
pediatrician told us not to worry. It wasn’t until my wife, Laurie,
started looking on the internet that she connected the
dots and diagnosed him with autism herself. It took me
longer to accept this. I had a lot of excuses for why he wasn't talking; his
older brother was talking for him, he was just
stubborn, he was independent. This actually delayed the
official diagnosis. He certainly didn't fit my picture of autism, which
basically came straight from "Rainman." They barely
mention autism in medical school. But after reading
the stories that Laurie found from other people, I had to admit that they
described our little boy.
Even though we knew he was autistic before we brought him in for an official
diagnosis, we weren't remotely prepared for what the psychiatrist told
us. He said, "Your son meets ten out of the twelve
criteria for full-blown autism. His prognosis is very
poor. He's likely to be institutionalized. You can put him in our school and
we'll try to teach him some skills, but it's unlikely
that he's ever going to achieve any kind of functional
level." Furthermore, he said, "Don't waste your time looking at alternative
treatments like diet and vitamins and things like that because they’re a
waste of money."
Since I was a very traditional allopathic physician, I didn't know that there
was any other way of thinking about autism. I thought
the only possible course was acceptance. I knew that
the day would never come when we would put him in an
institution, but I didn't realize that there was a lot more information about
autism than what we were being told. Laurie was not
willing to accept the prognosis and started
researching on the internet. I'm sure this is a story that many of you are
familiar with--she found the Autism Research Institute (ARI) website and she
started Aaron on a glutenand casein-free diet and
added B6 and other vitamins. She brought the information to
me. I assented because I thought that she needed to feel like she was
doing something and I knew it wouldn't hurt Aaron. But
when she started bringing me research papers about the
possible dangers of vaccines, I took notice. I said, "This is ridiculous.
Vaccines have nothing to do with autism." And I started reading the
research in order to prove her wrong and to show her
that I knew how to read research and she didn’t. To
make a long story short, here I am.
I became involved because I was told my son would be institutionalized, and
that was unacceptable. I also became involved because
there seemed to be a lack of knowledge about autism
among the medical community in my area. None of the
supposed autism experts or the pediatricians we consulted could give us any
answers. I became involved because what I was reading
and seeing in the medical literature and in my own son
and in other children was disproving or contradicting the mainstream dogma
of autism.
The History of Autism
Backtracking a little, I’d like to look at the history of autism. I
think the history of autism is like the parable of the
three blind men and the elephant. You all know the
parable I’m sure. The first blind man feels the trunk and says, “This is a
snake.” The second blind man feels the elephant’s leg
and says, “This is a tree.” The third blind man feels
the elephant’s tail and says, “This is a rope.” They don’t realize that they’re
feeling a much more complex organism. Autism is a lot
like that. In the history of autism there have been a
lot of blind men.
The first blind man’s name was Bruno Bettelheim. I’m sure that most of you
are aware of his “refrigerator mother” theory. He
claimed that children became autistic because they
withdrew in response to their cold, unloving mothers. Thanks to Bernard
Rimland and other people this theory was discredited, but it was the
mainstream theory for decades. As recently as 1981
Bettelheim said, “All my life, I have been working with
children whose lives were destroyed because their mothers hated them.”
This is what some of the experts believed about autism
even very recently.
Other blind men said that “Autism is a developmental disorder with
impairments in language and social interaction and
associated with repetitive, stereotyped behaviors.”
I’m sure you’re familiar with this; it is the current definition of autism in
the DSM IV (Diagnostic and Statistical Manual of
Mental Disorders). Well yes, it’s true. Autistic
children have developmental problems, but this is only one part of the organism
that we call autism and if you stop there, you’re
missing the boat. Other blind men say that autism is a
genetic illness. The implication is that nothing can be done because the
events leading to the disease happen very early in fetal development.
Autism is a genetic illness in that it has a genetic
component, a genetic susceptibility, but if you stop there
you’re also missing the boat.
The blind men can’t answer these questions: if autism is a genetic illness,
why is the incidence increasing so dramatically? If
autism is a behavior disorder, why do the children
have chronic bowel problems? Why do they have ear infections, frequent viral
infections, and eczema? Why do they have nutritional deficiencies? And
why do most autistic children seem to develop normally
and then start to regress? These are questions that
can’t be answered by their theories.
This illness was first described back in 1940. In 1940 doctors may not have
known as much about how to treat certain diseases, but they were very
good at describing them. That’s when most of the
illnesses that we now know about were first labeled.
Autism was unheard of and unreported before then. When Leo Kanner described it,
he said that neither he nor his colleagues had ever
seen autistic children before. Full-blown autism is
not a subtle disorder. Had it existed, it would have been described in the
medical literature.
It’s been more than sixty years since then. Where has the research been? We
have very little still. The only explanation I have for that is that
since it was considered to be a very rare genetic
disease, the government didn’t feel research merited funding.
Even now that we know that it’s not rare--the CDC acknowledges that more
than 1 in 166 kids are on the spectrum--there’s still
very little money going to autism research compared to
other diseases with similar incidence rates.
Here is a graph of the research dollars spent per patient in a variety of
disorders. In the US the number of patients affected
with AIDS and with autism are basically the same.
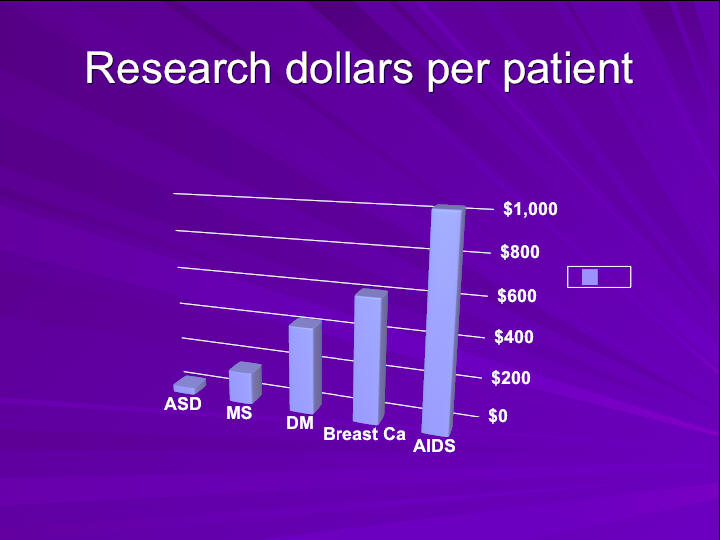 For every AIDS patient about one thousand dollars are spent and for every
autistic patient about forty dollars are spent. I
think AIDS, diabetes, breast cancer, and MS are very
important diseases, but if you look at the economics or the social cost to
society, autism trumps them all. The cost of caring
for all of our autistic children, and the cost of their
lost productivity, far outweighs any of these other disorders. Why are
the media and the government ignoring the problem? You
hear President Bush on the news talking about avian
flu or West Nile virus, and the possibility of an epidemic--well, we have an
epidemic of autism under our very noses. Why is this not on the front
page of every newspaper? Where is the research? Only
recently has the medical community been paying
attention to autism. It’s still too little and too late.
For every AIDS patient about one thousand dollars are spent and for every
autistic patient about forty dollars are spent. I
think AIDS, diabetes, breast cancer, and MS are very
important diseases, but if you look at the economics or the social cost to
society, autism trumps them all. The cost of caring
for all of our autistic children, and the cost of their
lost productivity, far outweighs any of these other disorders. Why are
the media and the government ignoring the problem? You
hear President Bush on the news talking about avian
flu or West Nile virus, and the possibility of an epidemic--well, we have an
epidemic of autism under our very noses. Why is this not on the front
page of every newspaper? Where is the research? Only
recently has the medical community been paying
attention to autism. It’s still too little and too late.
If you remember one thing from my lecture, I hope it’s this: you can make a
difference. Almost every significant advance that has ever happened for
autism has ultimately been the result of the efforts
of parents. This is not a disease that is going to be
cured from the top down. It’s going to be cured from the bottom up. The NAA
slogan for this conference is: “In order for us to
hear their voices, we must first raise ours.” NAA’s
mission is to bring awareness to this disease. Looking at the history of
government spending on autism research, we can’t
expect much unless we parents start making a
difference. The reason awareness is increasing now is because of the efforts of
all of you. We all have a part to play. We can’t just
focus on our own children, we have to help everybody
else’s children too.
Is There an Autism
Epidemic?
I think this is one of the most important questions that we need to
address. Unbelievably, it’s still being debated. Here
are the California statistics:
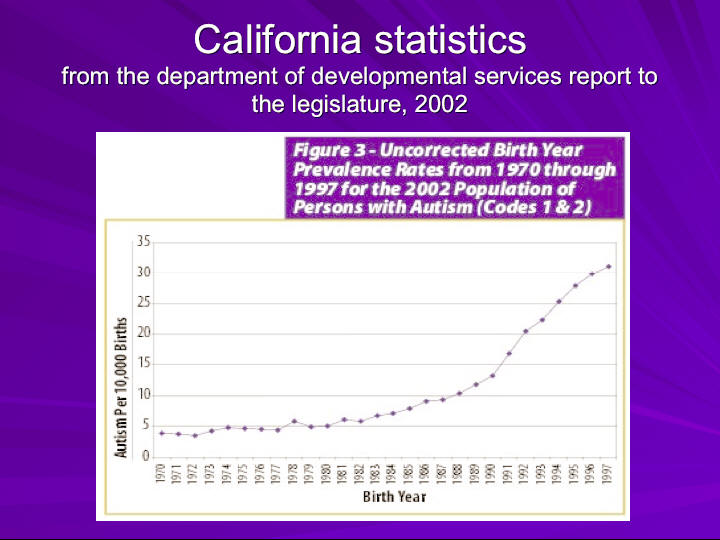
The reason we see California statistics so often is that they’ve been keeping
track of autism diagnoses longer than any other state,
since the 1970s. Most states started in the ‘90s when
it was mandated by the Department of Education.
From 1970 up until the mid-1980s it was a fairly flat line. It started to
rise in the mid ‘80s, and in the early ‘90s it spiked.
It’s important to mention that this is codes one and
two. In the autism diagnosing system these codes indicate full-blown
diagnostic criteria autism. Asperger’s syndrome and
PDD-NOS are not included in this graph, even though
their graphs look very similar. The graph above goes up to 1997. This one starts
in 1993 and goes up until July 2005:
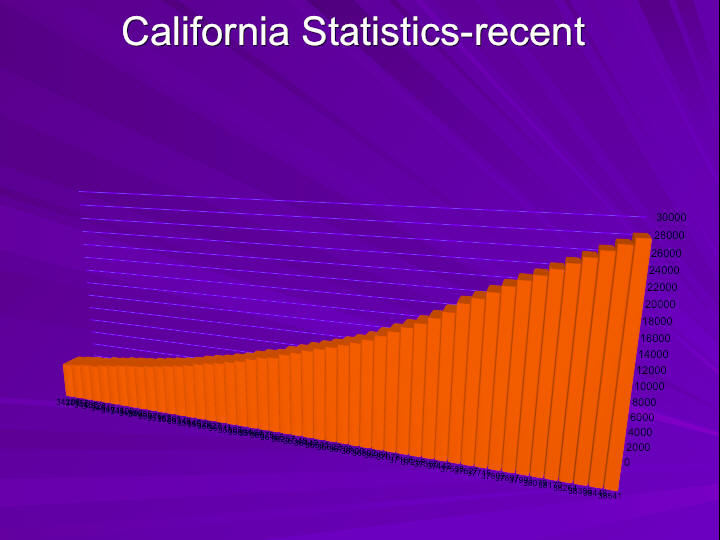
The curve keeps going up. If you look at this number at the top, it’s 28,000.
Back in the ‘70s, there were fewer than 100 cases in
California. Now there are 28,000 cases. They’re adding
more than 3,000 cases every year. There’s a theory that the reason that
California has so much autism is because computer geeks and engineers
with no social skills move to California and marry
each other and have a lot of autistic kids. The
proponents of this theory claim that California’s explosion in autism diagnoses
is specific to California.
I was tired of hearing this, so I decided to take the numbers from the
Department of Education for all the states and graph a
percent increase over a ten year period from
1992-2002:
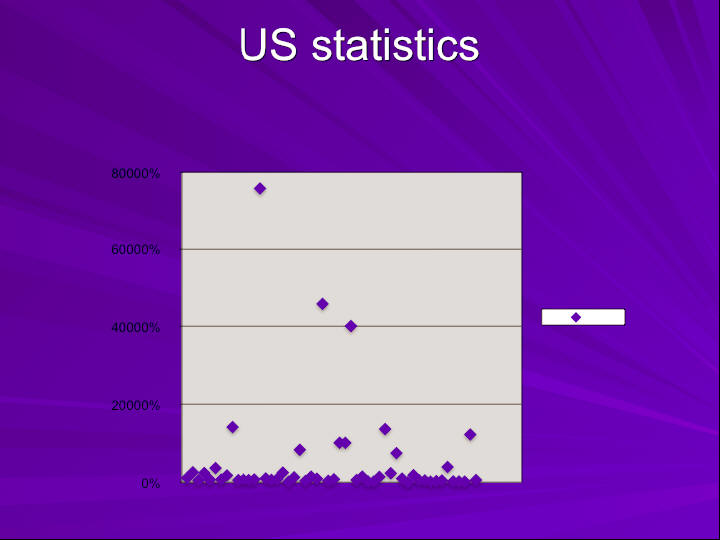 California is right in the middle. This is an exponential graph. The national
average is 714%, and California is average. Some of
the states at the top went from virtually no cases of
autism to thousands. This is a nationwide problem. And this is a problem of
developed countries. We don’t know about underdeveloped countries because
they don’t keep track.
California is right in the middle. This is an exponential graph. The national
average is 714%, and California is average. Some of
the states at the top went from virtually no cases of
autism to thousands. This is a nationwide problem. And this is a problem of
developed countries. We don’t know about underdeveloped countries because
they don’t keep track.
Is autism an epidemic? Autism experts say that the dramatic increase in
numbers is due to several factors: broader diagnostic
criteria, better diagnosis, or previous
misclassification of the disease. Some say it’s because more parents are
suddenly seeking services, giving misleading numbers.
Let’s look at each of those arguments. Has the diagnostic criteria changed
for autism? Yes, when the DSM IV came out in 1994
there was a change. They broadened the autism
spectrum. They included diseases like Asperger’s, PDD-NOS, Rett’s, and
CDD (childhood disintegrative disorder). They put them all under one
umbrella. But they actually defined true autism more
narrowly. If this argument was true, you would expect
a spike in the rates for the first couple of years after the DSM IV came out,
and then the rates would flatten out again. But that
didn’t happen. The numbers continued to rise.
California commissioned the MIND Institute at UC/Davis to study the
epidemiology in order to see if they could explain the dramatic increase.
They had several aims to their study. The first aim
was to determine whether the different criteria used
to diagnose autism explained the rise in the numbers. They looked at two groups,
one born in the 1980s and one born in the 1990s. They went back and they
re-diagnosed all of the kids based on the new criteria
to see if there was any difference. They found that
the change in diagnostic criteria could not account for the explosion.
The second study aim was to investigate whether the misclassification of some
cases of autism as mental retardation contributed to the apparent
increase. They took all of the kids in the study group
from the 80s and the 90s who had been diagnosed with
mental retardation and checked to see if any of the kids met the criteria for
autism. They found that 10-15% of the kids had
autistic characteristics as part of their mental
retardation syndrome. They found that in both groups there was some missed
autism, but there was no difference in the rates
between the two groups.i
Dr. Lisa Croen also looked at the California numbers. She said that autism
was increasing at the rate of 9% per year and mental
retardation was decreasing at about the same rate,
indicating that we’re substituting autism diagnoses for mental retardation.
Mark Blaxill, one of the founders of SafeMinds, reviewed her data and
showed that she was interpreting it incorrectly. When
the data for the true age of diagnosis for the two
conditions was corrected, it became apparent that mental retardation slowly
increased (as it has for many years), and that autism
was rising exponentially. He published his rebuttal
and Dr. Croen acknowledged that he was right.2,3
Are physicians better at diagnosing autism? Raise your hand if your doctor
was the first one to tell you that your child had
autism. Nobody? One? One. How many took your concerns
to your doctor and were ignored for several visits? Did they tell you,
“Boys will grow out of it,” or “Einstein didn’t talk until he was five,”
or “It’s because he has older siblings”? A myriad of
excuses. Physicians are not better at diagnosing autism.
Autism is a behavioral diagnosis. It doesn’t need CAT scans, it doesn’t
need labs, it doesn’t need improved technology. All
you need to diagnose autism is a history and a
physical exam. There’s no reason to suspect that twenty years ago doctors were
less able to take a history and do a physical exam. In
fact, I think it’s the other way around. I think most
doctors now rely too much on technology and have forgotten some of the
basic skills. It’s highly unlikely that twenty years ago a doctor with a
full-blown autistic patient in his office would say,
“There’s nothing wrong with this child.”
Most cases are still being referred through the education system or through
the continued persistence of the parents. My
experience has been that most physicians are still
inadequately educated about autism, but I will say that awareness is improving.
Unfortunately, most of the awareness has come because they’re so anxious
to convince you that vaccines are completely safe, but
I’m seeing many more kids getting an early diagnosis.
You would expect earlier diagnosis from increased awareness, but it’s not
going to change the total numbers in the community.
Were we missing cases in the old days? If the incidence has not increased,
then the rate of adults with full-blown autism is 1 in
250 or higher. This would mean that over 850,000
adults are currently affected (this does not include PDD-NOS and Asperger’s).
Now, if adults with full-blown autism are not treated, they do not get
better. They need social support, making them
responsible for a big drain on resources. If we apply the
numbers we see in our children to the adult population, there are over
one and a third million on the autism spectrum in the
US. Where are they all? If you wanted to find people
who are functioning poorly in society, you would look in homeless shelters,
prisons, and psych wards. Researchers combed these places looking for
individuals with undiagnosed autism. In fact, they did
find some, but at a rate of 1 or 2 per 10,000 which is
the rate at which autism was diagnosed back in the ‘70s and ‘80s--nowhere close
to the rate that we’re seeing today. There is no
“hidden horde” of undiagnosed autistic adults. Here is
a graph of the age distribution of all the patients that have autism in
California:
 If you look at the purple bars, this is the distribution back in 1987. At
that point from the age of 5 up until the age of 29
the bars were fairly flat, and then after that they dropped
off dramatically. Look now in December 2002--the gray bars--look how the
curve shifted to the left. Basically now a third of
the patients in California are between five and nine
years old. Eighty percent are younger than fourteen. All of a sudden an
explosion of autism skewed the percentages towards our
younger kids. All of those bars should be equal, if
there isn’t an epidemic.
If you look at the purple bars, this is the distribution back in 1987. At
that point from the age of 5 up until the age of 29
the bars were fairly flat, and then after that they dropped
off dramatically. Look now in December 2002--the gray bars--look how the
curve shifted to the left. Basically now a third of
the patients in California are between five and nine
years old. Eighty percent are younger than fourteen. All of a sudden an
explosion of autism skewed the percentages towards our
younger kids. All of those bars should be equal, if
there isn’t an epidemic.
I think the silliest argument is that there is an apparent increase because
more parents are seeking services. Autism represents a
significant financial and emotional drain on everyone
involved. Do they really think that 10 years ago parents were less
likely to look for help for their autistic kids than they are today?
Suddenly there were so many great services available
that parents started coming out of the woodwork to get
help? In the old days we didn’t go to the doctor, we didn’t go to the school, we
just stayed in our house. This is ridiculous. It is
unreasonable to assume that the parents of more than
3,000 children a year in California alone did not seek any services for level
one autism in previous years. It’s nonsensical, yet you hear it all the
time, and you read it in well-established,
well-respected medical journals.
We know that autism is an epidemic. Why does it matter? It matters because
there’s no such thing as a genetic epidemic. Ask any geneticist and
they’ll tell you that genes on their own can’t work
that fast. If autism is an epidemic, it has to have an
environmental component; there’s no other explanation. The fact that it’s an
epidemic matters because it’s going to guide our
research, it’s going to guide treatment, and it also
implies that there is treatment. It implies that there’s prevention, and it
implies that there’s a potential cure, so it makes all
the difference in the world.
Autism is a Medical
Disease
We need to shift our thinking to a new paradigm of autism. It’s an
illness that has a genetic susceptibility factor
exacerbated by an environmental trigger or a series of
environmental triggers. If you look at most of our medical illnesses, they fit
this model. Most illnesses, including diabetes, MS,
and all the other autoimmune and chronic illnesses
that are on the rise, fit this model. Even heart disease and some of the things
that we think of as genetic traits fit this model. I use the analogy of a
gun and a bullet. If you have a gun and a bullet, you
can keep them separate and you’re not going to cause
much harm, but if you put them together, it will lead to trouble.
Autism is a complex metabolic disorder involving multiple organ systems,
primarily the toxicological, immunological, gastrointestinal, and
neurological systems. These organ systems are probably
the most poorly understood and the most complicated of
any in our body, and they’re also the most tightly integrated. For instance,
more than 70% of the immune system is housed in the
gastrointestinal tract, so you can’t have a problem in
one and not the other. All of the neurotransmitters (the chemicals in your
brain) also exist in the gastrointestinal system, where they have
separate roles. The GI system is one of the main
barriers against neurotoxins. Everything is tightly connected.
Doctors like to specialize. We become cardiologists or
gastroenterologists, and then we don’t have to answer
all of the questions. Unfortunately the body doesn’t work that way.
You have to look at the body as a whole if you expect to make a
difference when you’re treating autistic children.
I’m going to describe each of these systems a little bit and discuss some of
the research indicating that they play a role in
autism. Autistic children are predisposed to
environmental toxicity because of underlying metabolic abnormalities. Dr. Jill
James published a very important paper: “Metabolic
biomarkers of increased oxidative stress and impaired
methylation capacity in children with autism.” She thought it would be
interesting to look at the metabolism of autistic children instead of
only looking at records and data. She found
impairments in the methylation cycle, a very critical part of
our body’s functioning. She found that because of this problem in the
methylation cycle, our children are predisposed to low
glutathione which prevents them from detoxifying
normally. She also found that by using some of the co-enzymes to support that
cycle (TMG, folinic acid, and methylcobalamin
injections--all non-pharmaceuticals), the block can be
reversed.4
The methylation cycle is very important: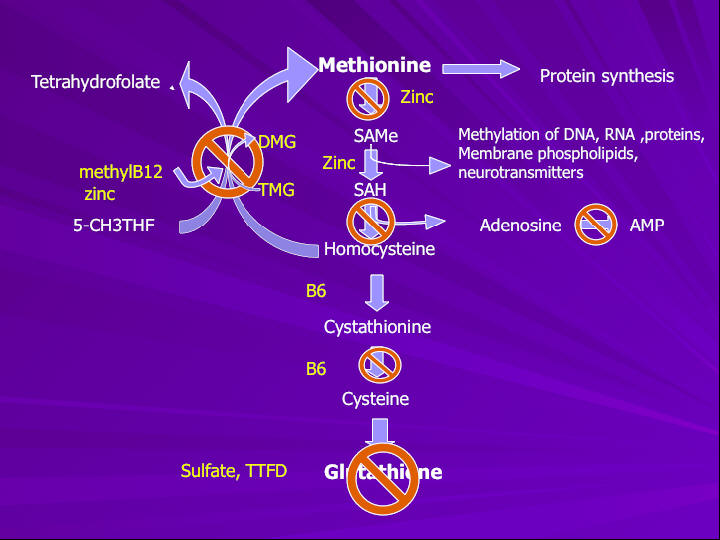
It explains a lot of what we think is happening in autism. Methyl is like the
body’s currency. It’s shuffled back and forth to
accomplish particular jobs and then it gets recycled.
These jobs include protein synthesis and methylation of DNA and RNA. It
turns genes on or off (making them active or inactive), helps to form
neurotransmitters, and helps to form cell membranes.
These are all fairly important tasks. It helps create
energy and then it can get recycled to form this molecule called glutathione.
Autistic children have blocks in several areas of this
pathway. The end result is that they’re not making
glutathione. If they’re not recycling it, they’re not sending out that methyl
group to do what it needs to do. Even before we
understood why, we noticed that a lot of kids improved
when we gave them B6, methyl B12 injections, zinc, or magnesium. These are
all co-factors in this pathway. When I talk about nutritional
intervention or multivitamins or minerals, it’s not
just because they seem like a good idea, but because they’re targeted
therapeutic interventions, not unlike a pharmaceutical.
Can low glutathione create problems with environmental toxicity? Most of the
time ER doctors leave biochemistry to the internists, but glutathione is
important in the emergency room because of Tylenol
overdoses. Tylenol is a very safe molecule unless you
take too much. It is metabolized in your body by glutathione. Our body renders
the Tylenol metabolite nontoxic and then we excrete
it. If you have taken too much Tylenol and it
overcomes the store of glutathione in your body, you can no longer metabolize
the Tylenol, it becomes toxic, kills your liver, and
then you die. The treatment for a Tylenol overdose in
the ER is to administer a precursor to glutathione called N Acetyl Cysteine.
Tylenol is just one example, but if you are already low in glutathione
it’s going to take a lot less of any toxin to cause
trouble. This makes sense. It explains why our children are
particularly vulnerable to environmental toxicity, even with toxins that
are relatively safe for other people.
Another important thing about glutathione is that it’s a major intracellular
antioxidant. Antioxidant means it helps prevent oxidative stress.
Oxidative stress is tissue damage that happens because
of the metabolism of certain molecules, especially
when they interact with oxygen in our body. Our body is set up to prevent
oxidative stress and tissue damage, but if you have
low levels of antioxidants you’re going to sustain
more damage. Glutathione
• prevents oxidation of cysteine residues in protein
• maintains mitochondrial integrity and ATP production
• maintains integrity of gut epithelium
• maintains normal T cell subsets and immune function
• stimulates SAM synthesis
• detoxifies heavy metals and other chemicals
• maintains vitamin C and vitamin E in active form,
so you can see it’s a very important molecule in our body.
The Role of Toxins
in Autism
We think that many of the symptoms of autism may be related to
problems caused by environmental toxins. We know
autism has some sort of environmental component, and
toxins can be neurologically damaging, so this is logical. Trying to correct the
underlying metabolic abnormalities and using methods to remove
environmental toxins can help our autistic children
get better.
The main question is this: what toxins are implicated in autism? Is it caused
by a single environmental insult, or an accumulation
of multiple insults? I, for one, do not believe that
it’s a single molecule, because autism is simply too complex. There are a lot
of people who believe that mercury is the cause of autism. I think that
mercury plays a role, but I don’t think that the
removal of thimerosal from vaccines will cause autism to
go away completely. In fact, I know it won’t because I’ve seen kids who
have not been exposed to thimerosal who are still
autistic.
I think the analogy of the straw that broke the camel’s back is the most
appropriate. Our autistic children are genetically vulnerable to start
with and then they are loaded with lots of “straw.”
Look at how toxic our environment has become. There
are 80,000 chemicals that have been introduced into the environment in the last
twenty years (the same period as the autism epidemic)
that have never been tested for neurological toxicity.
If you’re a child who can’t detoxify, any of those chemicals might
cause harm. The accumulation of multiple chemicals can act cumulatively
or synergistically, one making the other more harmful.
I think that that’s actually what we’re seeing in
autistic children.
Now, having said that, I want to talk about mercury. I want to make it clear
that there’s a lot of evidence indicating that mercury
is an important factor. The way that the thimerosal
issue is being handled by the government in determining research priorities is
not transparent. The only way that their behavior makes sense is if
they’re hiding something, and if they’re hiding
something I want to know what it is. If it turns out that
autism is not related to mercury, we can move on, but if it is related,
that information will help determine treatment for our
children. It will help prevent other children from
becoming autistic. I’m not interested in placing blame, I simply want the kids
to get better.
We know that mercury is very highly neurotoxic. In fact, I’ve been told that
it’s the most neurotoxic substance on earth that isn’t
radioactive. It’s dangerous to developing brains. It
impacts cognitive thinking, memory, attention, language, and fine
motor and visual-spatial skills. Sound familiar to any of you?
Concentrations are rising in the environment. Sources
include coal burning power plants, fish consumption, dental
amalgams, and medical products. Let’s go through the mercury cycle.
Methyl mercury is used in the refining process in
power plants. It is emitted into the air, goes up into the
atmosphere, comes down in the rain, and ends up in the ocean. At that
point it’s inorganic mercury. Algae in the ocean can
convert it to organic mercury, and then fish eat the
algae, bigger fish eat the smaller fish, and then we eat the bigger fish. It
becomes concentrated in the tissues because living
organisms can’t excrete it very well. The higher you
are on the food chain, the more mercury ends up in your system.
It has been shown that mercury can pass through the placenta and into the
fetus and cause damage. This is from the Environmental
Protection Agency’s website:
• “The developing nervous system of the fetus may be more vulnerable to
methyl mercury than is the adult nervous system.” (In
other words, the mothers may be asymptomatic while
their kids manifest neurological damage.)
• “630,000 of the roughly 4 million babies born annually in the US--twice as
many as previously thought--may be exposed to
dangerous levels of mercury in the womb.”
• “Given the new finding that umbilical cord blood has higher concentrations of
mercury, the EPA believes that the safe level for mercury in mothers’
blood is 3.5 parts per billion. About 15% of women of
childbearing age had blood levels that high, according
to the CDC study.”
One-sixth of pregnant women have high enough blood levels to cause brain
damage to their fetuses, just from methyl mercury.
That’s terrifying. Can it really be coincidence that
the CDC also reports that one sixth of our children have learning disabilities?
Here is another example of how a few parents can make a huge difference
in the world: Sallie Bernard and others started
looking at mercury and wondering if there might be a
connection to autism. They looked at historical cases and cases in the medical
literature and they listed all of the characteristics and the physiology
and the behaviors seen in methyl mercury poisoning. Lo
and behold, there are about 150 of them, and almost
all of them have something to do with autism. In fact a lot of them are almost
identical to traits of autism, both physiologically and behaviorally.
They published a paper called, “Autism: A Novel Form
of Mercury Poisoning.” 5
In 1998 the FDA finally noticed that our kids were getting too much mercury
in their vaccines. They realized that when the CDC
added hepatitis B and HiB to the vaccine schedule in
the early ‘90s, children were suddenly getting as much as two and a
half times more mercury than they had before. This was in the first six
months of life, which is the most critical time of
development. On a single day if a child was given four
or five vaccines, they would have received over 100 times the safe standard of
organic mercury based on oral ingestion guidelines for
adults.
The FDA encouraged the manufacturers to stop making mercury-containing
vaccines. They didn’t do a recall. A letter has recently surfaced in
which GlaxoSmithKline offered to provide mercury-free
vaccines immediately, but the government declined
their offer. Apparently they were perfectly comfortable waiting a
couple of years for all of the manufacturers to start producing
mercury-free vaccines, so mercury-containing vaccines
stayed on the shelves for years afterwards, at least until
2003 and probably beyond that.
There is still thimerosal in vaccines. Many Rhogam shots have thimerosal
(Rhogam is given to pregnant women). Flu shots have thimerosal in them.
There are thimerosal-free varieties of both of those
shots, but they’re not the common ones. The CDC now
recommends that all young children and pregnant women get flu vaccines.
Thimerosal is still in tetanus boosters. And there are still trace
amounts in many of the standard early childhood
vaccines. They still use thimerosal in the vaccines that they
ship overseas, so we’re exporting it to all of the developing countries.
(Coincidentally, there’s an explosion of autism in
developing countries.)
Thimerosal is nearly 50% ethyl mercury. Ethyl mercury is organic mercury, but
it’s different from methyl mercury. It’s used as a preservative to enable
the manufacturer to package their vaccines in
multi-dose vials. It was known to be toxic by the
manufacturer, Eli Lilly, when it was first developed. The original safety
studies were very poorly done. They tested thimerosal
in 1930 on 22 individuals, all of whom were sick with
meningitis. They all died. Lilly concluded that it was meningitis that killed
them, and that thimerosal was safe. That’s the safety study. That’s the
“science” that grandfathered it in for use in our
medical products.
The LA Times reprinted memos from the 1990s that show that Merck knew that
mercury levels in the vaccine schedule had become excessive, but
they chose to do nothing. Thimerosal was removed from animal
vaccines in the early 1990s because the veterinarians decided it
was too toxic. A bottle of thimerosal is legally required to
include a skull and crossbones on the label. It seems
unfathomable that anyone would take a substance requird to
carry this label and add it to baby vaccines.
 The CDC decided to investigate a possible connection
between thimerosal exposure and autism. Surprise--they decided
there was no connection. They were careful to consider only
epidemiological studies, specifically ones which had been
constructed to show no connection. 6,7, There was a lot of media
coverage and all of the pediatricians were relieved. But
SafeMinds looked at the data in detail and showed that all of the
studies were invalid because of inherent biases and data
misinterpretation.8,9,10 Some other epidemiology studies were
done by the Geiers and they found that thimerosal was related to
the increase in autism.11,12,13 The chance of developing autism went up
by as much as 21% in one of their studies. There’s a
lot more information on this controversy in David
Kirby’s book, Evidence of Harm, and there’s also a lot of information at
www.nomercury.org,
www.safeminds.org,
and
www.nationalautismassociation.org. Because
epidemiological studies can be manipulated so easily, they are not
ordinarily used to prove causation or lack thereof. It is accepted within
the scientific community that they are meaningful
primarily to indicate areas for further investigation.
The CDC decided to investigate a possible connection
between thimerosal exposure and autism. Surprise--they decided
there was no connection. They were careful to consider only
epidemiological studies, specifically ones which had been
constructed to show no connection. 6,7, There was a lot of media
coverage and all of the pediatricians were relieved. But
SafeMinds looked at the data in detail and showed that all of the
studies were invalid because of inherent biases and data
misinterpretation.8,9,10 Some other epidemiology studies were
done by the Geiers and they found that thimerosal was related to
the increase in autism.11,12,13 The chance of developing autism went up
by as much as 21% in one of their studies. There’s a
lot more information on this controversy in David
Kirby’s book, Evidence of Harm, and there’s also a lot of information at
www.nomercury.org,
www.safeminds.org,
and
www.nationalautismassociation.org. Because
epidemiological studies can be manipulated so easily, they are not
ordinarily used to prove causation or lack thereof. It is accepted within
the scientific community that they are meaningful
primarily to indicate areas for further investigation.
They are not conclusive on their own. Is there biological plausibility? Is
thimerosal neurotoxic? Parran14, Mutkus15, and
Baskin16 have published three different research
studies proving that thimerosal causes death in brain cells.
Mady Hornig at Columbia University did a study on mice.17 She injected
several groups of mice with thimerosal approximating
the exposure our infants would have received on the
CDC’s recommended vaccine schedule. Some of the mice were
genetically predisposed to autoimmune disorders. What she found was that
most of the mice were fine, but in the group of mice
who were predisposed to autoimmune disorders,
thimerosal caused social withdrawal and repetitive activity. She found brain
damage very similar to what we see in the brains of
individuals with autism.
Thomas Burbacher did an extremely important study on infant monkeys.18 His
study compared oral ingestion of methyl mercury with ethyl mercury
injected into the muscle. He gave one group oral
methyl mercury, simulating fish consumption, and
injected the other group with thimerosal, simulating a vaccine exposure. He
found that ethyl mercury left the blood stream very
rapidly. That was very reassuring to most people,
because methyl mercury takes 20-30 days to leave the blood stream.
The CDC sent out a big press release saying that ethyl mercury was much
safer than methyl mercury because it left the blood
stream after seven days. The part of the study that
they didn’t mention was the part that showed what happened to ethyl mercury
once it left the blood stream. It crossed the blood-brain barrier, was
converted into inorganic mercury, and became lodged in
the brain. The half-life of inorganic mercury in the
brain is 20 + years. That part wasn’t publicized, but it’s right there in the
study--you can read it. An important conclusion
Burbacher reached was that the safety of ethyl mercury
could not be determined by methyl mercury studies. He called for further study
of ethyl mercury to assess true toxicity. Currently all of the government
safety standards are based on methyl mercury.
The Havarinasab study showed that mercury compounds, particularly inorganic
mercury, can induce autoimmune reactions.19 (Remember that thimerosal
converts to inorganic mercury.) Autistic children have
autoimmune reactions, so it would be logical to
investigate whether or not they have a problem excreting mercury. Jill James did
a study looking at thimerosal neurotoxicity associated
with glutathione depletion. She showed that autistic
children have impaired methylation and low glutathione, and
thimerosal depletes glutathione in brain cells making them prone to
damage. Glutathione helps to detoxify thimerosal and
if you’re exposed to thimerosal it’s going to deplete your
glutathione levels even further.20
Drs. Waly and Deth showed that thimerosal can interrupt methylation by
interfering with methionine synthase.21 This is one of the enzymes that
is in the methylation cycle. Methyl B12 is effective
because it helps repair the disruption in methionine
synthase. Thimerosal might be why our kids are having trouble with the
methylation cycle.
Dr. Amy Holmes published a study in the Journal of Toxicology in 2003.22 She
tested the baby hair of children who were later diagnosed with autism.
Hair is a measure of excretion. She compared the hair
with hair from neurotypical (“NT”--developmentally
normal) controls. She showed that with a comparable mercury exposure, the
autistic children had less mercury coming out in their
hair. At that time we had very little understanding of
the impairment in the detoxification system of affected children, so the
results surprised her. She expected more mercury to come out, reasoning
that if kids are mercury-toxic they should have a lot
of mercury in their body. The fact that these kids
have significantly less mercury coming out in their hair than NT children makes
perfect sense to us now, because we suspect they’re
storing it.
Dr. Bradstreet did a study comparing the results of an oral challenge with a
chelator called DMSA in a group of autistic children compared with NT
controls.23 The children with autism excreted a lot
more mercury when using a chelator than the NT
children did, also suggesting that they were retaining mercury. Do autistic
children improve with mercury removal therapy? We
think the answer is yes. There’s a lot of anecdotal
evidence to that effect. To be honest, we’re lacking strong research studies. In
an open trial of chelation with DMSA and lipoic acid in children with
autism--an observational study in their practice--Dr.
Jane El-Dahr, Dr. Amy Holmes, and Dr. Stephanie Cave
found that of the 152 kids with autism whom they chelated, the vast
majority improved. Here are their results:
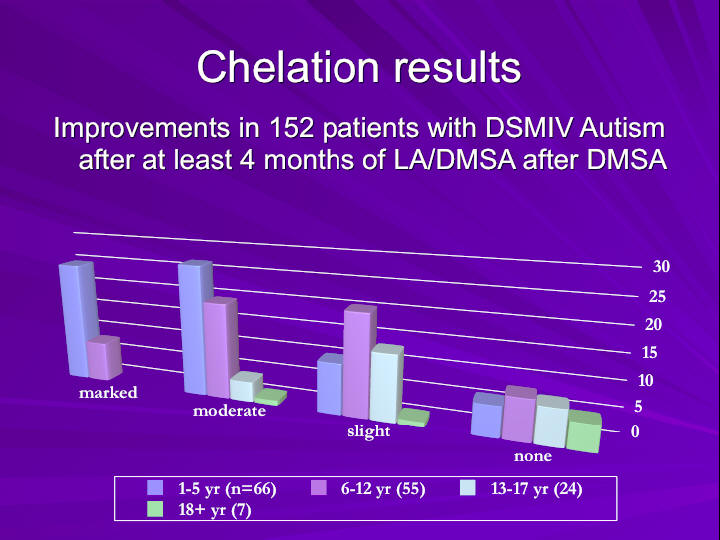
They also found that the younger children seemed to improve from chelation
much more dramatically during this time frame than did
the older children.
ARI asks parents to assess the effectiveness of various treatments. They have
data from 23,000 parents of autistic children. 73% of the parents who
responded felt that their children improved with
chelation, 25% reported no change, and 2% got worse.
Compare that to Ritalin: 29% reported improvement, 26% reported no change, and
44% said their children got worse. Yet most of your
pediatricians are happy to prescribe Ritalin--and
they’re critical of people who are doing chelation because they claim it’s
dangerous. Jim Adams is currently doing a double-blind,
placebo-controlled study of chelation effects on
autistic children using DMSA. Based on what I’ve seen in my
practice, I think this is going to be an important study and I think it’s
going to see an effect.
The CDC asked the IOM (Institute of Medicine) to investigate the
autismthimerosal connection, so the IOM met and
reviewed all of the literature, including the studies
that I showed you. A couple of the studies weren’t out yet, including the
Burbacher study. The IOM knew these studies were about to come out but
decided not to wait. Their conclusion was that based
on the epidemiological studies showing no
relationship, no further studies should be done regarding thimerosal and autism.
From a purely scientific point of view, does that make
sense? We have a lot of biological evidence about
mercury toxicity, we have evidence that it can cause autistic-like
behavior, we have evidence that shows the damage it can cause in the
brain cells, we have evidence that shows that autistic
children have trouble with mercury in particular--but they announced that no
further research was necessary in this area, and funding
would not be forthcoming. I’ll let you draw your own conclusions.
4/21/06 addendum:
A recent study at the MIND Institute at UC Davis looked at the response of
dendritic cells to a brief exposure of minute amounts
of thimerosal.58 Dendritic cells act in the immune
system as antigen presenting cells, which means that they take a foreign
molecule, package it, and present it for the T-cells (killer cells) in
the immune system to recognize and deal with
appropriately. The study demonstrated that these cells are
extremely sensitive to thimerosal-induced damage, leading to cell death
at higher concentrations and cell dysfunction at lower
concentrations of thimerosal exposure. Thimerosal also
affected the secretion of cytokines, which are the chemical messengers
of the immune system, resulting in an immediate exaggerated response
followed by chronic immune suppression. It was also
clearly shown that it was the ethylmercury component
of thimerosal that caused the damage. The results of this study are potentially
important to further our understanding of the role of thimerosal in
causing or contributing to the immune abnormalities
seen in autistic children. The implication is that thimerosal
may have damaged their immune system and prevented them from responding
normally to viruses and other toxins. Interestingly,
dendritic cells are the site where measles virus is
normally found in tissue biopsies.
Gastrointestinal disease and immune dysregulation.
Children with autism frequently have gastrointestinal problems, particularly
constipation and diarrhea.24 When a child has GI symptoms, we generally
find inflammation somewhere along the GI tract, but
particularly in the terminal ileum, on endoscopy as
well as biopsy.25 Many autistic children have evidence of abnormal
intestinal permeability or what we call “leaky gut.”26 We continually
find inflammatory bowel disease that is different from
Crohn’s disease and ulcerative colitis.27 This was
initially named “autistic enterocolitis” by Dr. Wakefield because of the unique
pattern of inflammation.28 Articles are published in
the media all the time saying that what was seen in
the first 12 children in the Wakefield/Lancet study has never been duplicated.
In fact, it has been duplicated by independent sources
in hundreds and hundreds of kids now and has also been
reported in the literature, and yet it’s being ignored.29,30,31,32,33,34
Undiagnosed abdominal issues are the cause of many of the behavior symptoms
of autism. If you imagine yourself as a non-verbal or poorly
communicative individual who has chronic or
intermittent abdominal pain, a lot of your behaviors are going to look
pretty autistic. One example is abnormal posturing. We see some children
go to great lengths to put pressure on their lower
abdomen. They’ll lie on the corner of a table or the
arm of a sofa for hours. This was once considered an autistic behavior, but we
now know that it’s done exclusively to ease pain. What
we’ve learned is that when you treat the abdominal
symptoms, a lot of what were considered autistic behaviors disappear.
We think that the inflammatory process in the bowel may result in secondary
inflammation in the brain.35 This is an important study that has come out
recently:
“Neuroglial Activation and Neuroinflammation in the Brain of Patients with
Autism.” Diana Vargas documented that autistic
individuals have inflammation in the brain. This was
one of the first studies to show this, because the inflammation doesn’t show up
on MRIs or CAT scans, but it does show up on biopsies
of the brain (samples were taken from autistic
individuals who had died.) The pattern of the inflammation is not consistent
with the brain as the primary source. This is critical, because it
suggests that the inflammation is starting somewhere
else and the brain is a secondary target organ, not the
primary source. If we can isolate the primary source, we have a target
for treatment. Wakefield hypothesized just this--that
the brain encephalopathy of autism may be secondary to
an immune-mediated gastrointestinal abnormality, possibly mediated by
opioid peptides and/or a chronic viral source.
Autistic children have abnormal immune function including low natural killer
cell function and a TH1/TH2 imbalance.36,37 This means
that affected children are much more likely to develop
allergies and antibodies and a lot less able to kill off infections.
They have chronic inflammation and autoimmune reactions. Many of them
have eczema, chronic runny noses, ear infections--they
seem to be sick all the time. I also see kids on the
other end of the spectrum who never get sick. Even though the rest of the family
is sick, they’re fine. This suggests a hyper-immune
state. These are the kids who are more likely to have
auto-antibodies. The body attacks itself because the immune system is on
hyper drive.
Do the immune system and the gastrointestinal system interact? I mentioned
before that 70% of the immune system is located in the gut, so if you
have a leaky gut and an abnormal GI tract you’re going
to have abnormal immune status.38,39 Exposure to
common foods results in allergic reactions and creates chronic
inflammation.40,41,42 Dietary interventions
help--there are many studies supporting this.43,44,45, 46,47 With
exclusionary diets, such as the gluten and casein-free diet or the
specific carbohydrate diet, children improve as you
eliminate some of the things against which they’re reacting.
Jim Adams completed a study showing that many autistic children respond
to multivitamin/multimineral therapy.48 You hear
criticism of biomedical physicians who are treating
autistic kids with vitamins. And yet mainstream medicine recognizes that
some illnesses must be treated nutritionally. For example, alcoholism.
Alcoholics have nutritional problems. In order to
avoid brain encephalopathy, alcoholics need thiamine,
folate, and multivitamins. Any doctor would be happy to prescribe these because
they know that they make a difference. Another example
is short bowel syndrome, in which the patient doesn’t
have enough bowel to absorb nutrients. In any disease process that is
inhibiting the body’s ability to absorb or utilize vitamins,
supplementation is paramount. Vitamins are the
co-factors for our energy. We need them for our metabolic system to
work. And if you have a deficiency, it causes disease.
How do the immune system and the neurological system interact? We already
talked a little bit about this when we looked at the Vargas study49, but
what about viruses? The immune cell patterns in
children with autism are consistent with a viral
mechanism.50 Does measles virus play a role?51,52 This is one of the biggest
controversies in autism. All of the epidemiological studies seem to say
no, but again they have significant design flaws. We
continue to find vaccine-strain measles virus in the
cerebrospinal fluid and in the enlarged lymph nodes in the bowels of autistic
children and not in controls.53,54,55,56 MMR
antibodies are associated with anti-brain autoimmune
antibodies in autistic children.57 Does that mean that MMR is the cause
of autism? We don’t know, but it is associated, and
since measles virus is not present in NT kids, it
merits further study.
Here is an emerging model for autism: I call it the multiple-hit hypothesis.
Imagine an embryo with genetically susceptible chromosomes that prevent it from
detoxifying normally. The embryo will be exposed to things like mercury from
maternal fish consumption and maternal amalgams, mercury from its mother’s flu vaccine
and possibly her rhogam shot, antibiotics given to the mother, and other placental
toxins that we don’t even know about. Babies need to be able to detoxify almost from
conception. Children born between 1991 and 2003 were hit with 25 mcg of ethyl mercury in
the hepatitis B shot the day they were born. Some are exposed to antibiotics
soon after birth. Babies are exposed to toxins in breast milk. (I certainly don’t mean that
you should stop breast-feeding because there are many more benefits than risks, but the
reality is that it’s an exposure to toxins. I’m sure that there are toxins in formula as well).
All of these exposures start to weaken the immune system of a susceptible child, creating
early inflammation. They start to accumulate some of the toxins that they can’t get
rid of. Remember that the immune system and the detoxification system really take six
months before they start to become mature. As the child gets older, he or she receives
many more immunizations. Food antigens are introduced, like casein from cow’s milk.
They get repeated viral infections. They develop chronic ear infections and are given
multiple courses of antibiotics. The antibiotics damage their gut even more, allowing
more toxins to enter their system.
So the child is developing a leaky gut, tissue damage is getting worse, the
immune system is growing weaker, and autoimmune reactions are starting. Then a lot of
kids experience a catastrophic event. Either in the form of a significant illness or
a live virus vaccine. The immune system is overwhelmed and the child rapidly goes downhill.
Plenty of parents report a gradual deterioration, but many kids seem to develop
autism after a particular event. They go into the hospital or they get an MMR shot and
they’re never the same again. But I don’t think that the illness or the shot is the only
cause, I think autism is the end result of this developing series of reactions.
Autism is Treatable
Here is a list of some of the biological impairments in autism that we’re
aware of:
• Chronic diarrhea/constipation
• Yeast/bacterial overgrowth of bowels
• Inability to clear heavy metals
• Impaired sulfation
• Leaky gut syndrome
• Imbalanced immune system
• Mineral deficiencies (zinc, magnesium, selenium)
• Malabsorption/malnutrition
• Impaired neuronal development
• Disrupted hippocampus/amygdala
• Gluten/casein sensitivity
• Impaired secretin signaling
• Impaired detoxification
• Impaired antioxidation
• Omega-3 fatty acid deficiency
• Significant food allergies
• Impaired pancreatic function
• Frequent viral and bacterial infections
• Vitamin deficiencies
• Autoimmunity
• Neurotransmitter imbalance/dysfunction
• Sensitivity to vaccinations
• Seizures
• Impaired methylation
The definition of “biomedical treatment” is medical treatment which addresses
all of these issues. We look at the body from the biochemical perspective and attempt
to treat the root cause rather than just patch a band aid on the symptoms. Psychotropic
medications (Prozac, etc.) will not heal your children, they will only mask the
symptoms of their poor health. Biomedical intervention is not alternative. We run tests
to determine the source of dysfunction, and then we treat. I do not consider myself
an alternative practitioner. I’m a mainstream, traditional doctor, and this is
mainstream biochemistry--there is no such thing as alternative biochemistry. The research
I’ve discussed today is simply cutting edge, and most doctors haven’t taken the time
to look into it or to try to understand it.
When we treat the kids we correct their nutritional abnormalities. We treat
the gut. We support their own detoxification system. We remove the toxins from their
bodies. We break the inflammatory cycle. We support their immune system. We
treat for viruses. We try to heal the tissues. And we teach them. I mention teaching
because I think there’s a misconception among a lot of people even within the autism
community that either you seek biomedical treatment or you do ABA therapy. It’s not
either/or, it’s both. You must remove the barriers medically, and simultaneously you have to
teach the children. They have to be caught up to the stage their peers have achieved
naturally. Education and medical treatment work hand in hand.
This is the new paradigm in autism: autism is an environmental illness with a
genetic component. It’s a complex metabolic disease, not just a developmental
disability. It involves multiple body systems that are interacting with each
other. Autism is treatable. That’s an important message to hear for those of you who are just
starting out, but I think it’s equally important for those of you who’ve been struggling
for years and years and still have a long way to go. It’s a marathon, it’s not a sprint.
Autism is a very complicated illness. There’s still a lot we don’t know, but our
understanding is improving. You’ll hear some parents say that their children virtually recovered
after a single intervention. But for most of us, myself included, it’s a long process.
It may take 100 interventions, it might take 10 or 15 years, and it will drain your
resources and your emotions. But the important thing is to never give up. Our children are trapped
in there and we have to fight to get them back out.
The other important thing is that we must continue to fight for a cure. I
said at the beginning of this talk that answers won’t come from the top down, but from the
bottom up. Until we raise our voices loud enough to change the thinking of those in
charge, we’re not going to make much progress. Until we have a government that is
willing to look for the cause, we’re not going to have the answers. We all need to play a
role. I believe that a cure is possible and I believe that autism can be prevented, but
it’s going to take a lot of work from all of us.
I’d like to briefly tell you about Thoughtful House. The part of my story I
didn’t mention earlier is that after I started learning about autism I opened up a
clinic called Children’s Biomedical Center of Utah. Ultimately I was intrigued by the idea of
combining medical care, education, and research, and I accepted Dr. Wakefield’s
invitation to join Thoughtful House. While we’re treating kids we’re also doing
research studies for mainstream medical journals so that all of your pediatricians and
family doctors will be more aware of what’s going on.
In closing, I’d like to leave you with one thought. One of the many annoying
things that my autistic son likes to do is to scribble on the wall. Most of the
time it’s just a random scribble of color, but once there was a small rainbow down at the
bottom of the wall. It reminds me that in spite of everything that we go through with our
children, we have to remember to look for the rainbows.
1. MIND institute: Report to Legislature on the principle findings from the
epidemiology of autism in California: a pilot study. Oct 17, 2002.
www.mind.org
2. Croen LA et al. The changing prevalence of autism in California. JADD
2002;32(3):207-215.
3. Blaxill MF et al. Commentary: Blaxill, Baskin, and Spitzer on Croen et al.
(2002), The changing prevalence of autism in California. JADD
2003;33(2):223-226.
4. James SJ, et al. Metabolic biomarkers of increased oxidative stress and
impaired methylation capacity in children with autism. Am J Clin Nutr
2004;80:1611-7.
5. Bernard S et al. Autism: a novel form of mercury poisoning. Med Hypothesis
2001;56(4):462-471.
6. Verstraeten T et al. Safety of thimerosal-containing vaccines: a two-phased
study of computerized health maintenance organization databases. Pediatrics
2003; 112(5):1039-1048.
7. Hviid, A, et al. Association between thimerosal-containing vaccine and
autism. JAMA 2003; 290(13):1763-1766.
8.
Danish Thimerosal-Autism Study in Pediatrics: Misleading and Uninformative
on Autism-Mercury Link by Mark Blaxill,
Director, Safe Minds report. 2003;
www.safeminds.org.
9. Bernard, S. Analysis of the Danish autism registry data base in response to
the Hviid et al Paper on Thimerosal in JAMA (October, 2003). Safe Minds
report 2003; www.safeminds.org.
10. Safe Minds report. A Brief Review of Verstraeten’s “Generation Zero” VSD
study results. 2003, www.safeminds.org.
11. Geier MR, Geier DA. Thimerosal in childhood vaccines, neurodevelepmental
disorders, and heart disease in the United States. J Am Phys and Surg
2003;8(1): 6-11.
12. Geier MR, Geier DA. Neurodevelopmental disorders after thimerosalcontaining
vaccines: a brief communication. Exp Biol Med 2003;228:660-
664.
13. Geier DA, Geier MR. A comparative evaluation of the effects of MMR
immunization and mercury doses from thimerosal-containing childhood
vaccines on the population prevalence of autism. Med Sci Monit
2004;10(3):P133-39.
14. Parran DK et al. Effects of thimerosal on NGF signal transduction and cell
death in neuroblastoma cells. Tox Sci 2005.
15. Mutkus L et al. In vitro uptake of glutamate in GLAST- and GLT-1-transfected mutant DHO-K1 cells is inhibited by the ethylmercury-containing
preservative thimerosal. Bio Trace Element Res. 2005;105:71.
16. Baskin et al. Thimerosal induces DNA breaks, caspase-3 activation,
membrane damage, and cell death in cultured human neurons and fibroblasts.
Toxicol Sci 2003;74:361-368.
17. Hornig M et al. Neurotoxic effects of postnatal thimerosal are mouse strain
dependent. Mol Psych 2004:1-12.
18. Burbacher TM et al. Comparison of blood and brain mercury levels in infant
monkeys exposed to methylmercury or vaccines containing thimerosal. Env
Health Persp 2005; 113(8):1015-21.
19. Havarinasab S, Hultman P. Organic mercury compounds and autoimmunity.
Autoimmunity Rev 2005;4:270-275.
20. James SJ et al. Thimerosal neurotoxicity is associated with glutathione
depletion: protection with glutathione precursors. Neurotoxicol 2005;26:1-8.Mol Psych 2004; 1-13.
21. Waly M et al. Activation of methionine synthase by insulin-like growth
factor-1 and dopamine: a target for neurodevelopmental toxins and thimerosal.
22. Holmes AS et al. Reduced levels of mercury in first baby haircuts of
autistic children. Int J Tox 2003;22:277-285.
23. Bradstreet J et al. A case control study of mercury burden in children with
autistic spectrum disorders. J Am Phys and Surg. 2003;8(3):76.
24. Afzal N et al. Constipation with acquired megarectum in children with
autism. Pediatrics 2003;112(4):939-942.
25. Horvath K et al. Gastrointestinal abnormalities in children with autistic
disorder. J Pediatr 1999;135:559-63.
26. D’Eufemia P et al. Abnormal intestinal permeability in children with autism.
Acta Paediatr 1996;85:1076-9.
27. Torrente F et al. Focal-enhanced gastritis in regressive autism with
features distinct from Crohn’s and Helicobacter Pylori gastritis. Am J Gastr
2004;doi:10.111;j.1572-0241.2004.04142.x: 598-605.
28. Wakefield AJ et al. Enterocolitis in children with developmental disorders.
Am J Gastroenterol 2000;95(9):2285-2295.
29. Wakefield AJ et al. Ileal-lymphoid-nodular hyperplasia, non-specific
colitis, and pervasive developmental disorder in children. Lancet 1998;351:637.
30. Wakefield AJ, et al. The significance of ileo-colonic lymphoid nodular
hyperplasia in children with autistic spectrum disorder. Eur J Gastr Hepatol
2005;17:1-10.
31. Ashwood P et al. Intestinal lymphocyte populations in children with
regressive autism: evidence for extensive mucosal immunopathology. J Clin
Immunol 2003;23(6):504-517.
32. Furlano RI et al. Colonic CD8 and gamma-delta T-cell infiltration with
epithelial damage in children with autism. J Pediatr 2001;138:366-72.
33. Ashwood P et al. Spontaneous mucosal lymphocyte cytokine profiles in
children with autism and gastrointestinal symptoms: mucosal immune
activation and reduced counter regulatory interleukin-10. J
Clin Immunol 2004;24(6): 664-673.
34. Torrente F et al. Small intestinal enteropathy with epithelial IgG and
complement deposition in children with regressive autism. Mol Psychiatry
2002;7:375-82.
35. Wakefield AJ et al. Review article: the concept of entero-colonic
encephalopathy, autism and opioid receptor ligands. Aliment Pharmacol Ther
2002:16:663-674.
36. Jyonouchi H et al. Proinflammatory and regulatory cytokine production
associated with innate and adaptive immune responses in children with autism
spectrum disorders and developmental regression. J Neuroimmunol
2001;120:170-179.
37. Krause I, et al. Brief Report: Immune factors in autism: a critical review.
JADD 2002;32(4): 337-345.
38. Jyonouchi H et al. Dysregulated innate immune responses in young children
with autism spectrum disorders: their relationship to gastrointestinal
symptoms and dietary intervention. Neuropsychobiology 2005;51:77-85.
39. Jyonouchi H et al. Innate immunity associated with inflammatory responses
and cytokine production against common dietary proteins in patients with
autism spectrum disorder. Neuropsychobiology 2002;46:76-84.
40. Jyonouchi H et al. Evaluation of an association between gastrointestinal
symptoms and cytokine production against common dietary proteins in
children with autism spectrum disorders. J Pediatr 2005;146:605-610.
41. Lucarelli S, et al. Food allergy and infantile autism. Panminerva Med
1995;37:137-41.
42. Vojdani A et al. Immune response to dietary proteins, gliadin and cerebellar
peptides in children with autism. Nutr Nueruosci 2004;7(3):151-161.
43. Reichelt KL et al. Probable etiology and possible treatment of childhood
autism. Brain Dysfunc 1991;4:308-319.
44. Reichelt KL, Knivsberg AM. Can the pathophysiology of autism be explained
by the nature of the discovered urine peptides? Nutr Neurosci 2003;6(1):19-
28.
45. Knivsberg AM et al. A randomized, conrolled study of dietary intervention in
autistic syndromes. Nutr Neurosci 2002;5(4):251-261.
46. Knivsberg AM, et al. Autistic syndromes and diet: a follow-up study. Sc J Ed
Res 1995;39(3): 223-236.
47. Knivsberg AM et al. Reports on dietary intervention in autistic disorders.
Nutr Neurosci 2000;4:25-27.
48. Adams JB, Holloway C. Pilot study of a moderate dose multivitamin/mineral
supplement for children with autistic spectrum disorder. JACM 2004;10(6):
1033-1039.
49. Vargas, DL et al. Neuroglial activation and neuroinflammation in the brain
of patients with autism. Ann Neurol 2005;57:1-15.
50. Uhlmann V et al. Potential viral pathogenic mechanism for new variant
inflammatory bowel disease. J Clin Pathol: Mol Pathol 2002;55:0-6.
51. Stott C et al. MMR and autism in perspective: the Denmark story. J Am Phys
Surg 2004;9(3):89-91.
52. Kawahima H et al. Detection and sequencing of measles virus from
peripheral mononuclear cells from patients with inflammatory bowel disease
and autism. Dig Dis Sci 2000;45(4):723-29.
53. Singh VK, et al. Abnormal measles-mumps-rubella antibodies and CNS
autoimmunity in children with autism. J Biomed Sci 2002;9:359-364.
54. Bradstreet JJ et al. Detection of measles virus genomic RNA in cerebrospinal
fluid of three children with regressive autism: a report of three cases. J Am
Phys Surg 2004;9(2):38-45.
55. Bradstreet JJ et al. Detection of measles virus genomic RNA in cerebrospinal
fluid of three children with regressive autism: a report of three cases. J Am
Phys Surg 2004;9(2):38-45.
56. Ashwood P et al. Detection of measles virus antigen in children with
autistic enterocolitis. In press.
57. Singh VK, Jensen RL. Elevated levels of measles antibodies in children with
autism. Pediatr Neurol 2003;28:1-3.
58. Goth, et al. Uncoupling of ATP-mediated calcium signaling and dysregulated
IL-6 secretion in dendritic cells by nanomolar thimerosal. EHP online March
2006 doi:10.1289/ehp.8881 (available at http://dx.doi.org/)